Public Opinion on Health Reform is Moving left for both R’s and D’s.
Posted on | January 24, 2019 | Comments Off on Public Opinion on Health Reform is Moving left for both R’s and D’s.

Mike Magee
If there is a face for a “compassionate capitalist”, many would drop in the wise visage of Warren Buffett who famously declared “Medical costs are the tapeworm of American economic competitiveness.”
Others have stated it differently while agreeing with results of the 2018 Bloomberg health efficiency index placing the U.S. dead last. The problem is systemic and nearly everyone knows it by now. Legendary Princeton health economist Uwe Reinhardt said as much declaring “At international health care conferences, arguing that a certain proposed policy would drive some country’s system closer to the U.S. model usually is the kiss of death.”
If most experts are there, where is the rest of the American public when it comes to a fundamental reboot of our inequitable and wasteful system focused on cure over care and profit over just about everything else?
The quick answer is, “They’re moving left at a pretty fast clip.” That’s the underlying message in a just released poll from the Kaiser Family Foundation. The report states that “Medicare-for-all starts with net favorability rating of +14 percentage points (56% who favor it, minus 42% who oppose it). This jumps to +45 percentage points when people hear the argument that this type of plan would guarantee health insurance as a right for all Americans.”
And this includes growing Republican support. Look at these numbers:
- 77 percent of the public, including most Republican (69%), favor allowing people between the ages of 50 to 64 to buy health insurance through Medicare;
- 75 percent, including most Republicans (64%), favor allowing people who aren’t covered by their employer to buy insurance through their state’s Medicaid program;
- 74 percent, including nearly half of Republicans (47%), favor a national government plan like Medicare that is open to anyone, but also would allow people to keep the coverage they have if they want to; and
- 56 percent, including nearly a quarter of Republicans (23%), favor a national plan called Medicare-for-all in which all Americans would get their insurance through a single government plan.
What are the concerns.
First, cost in the form of higher taxes. Most want to be assured that there will be substantial front end savings with universal coverage. That means simplifying insurance billing so that we no longer have 16 people employed for every physician in America.
Second, efficiency. Americans need to be reassured that universal coverage will not fundamentally undermine basic access to essential services.
Third, lower drug costs. People have grown tired of their politicians protecting well-heeled donors. They want action.
What would break the log jam in currently drugged-up America?
First, outlaw direct-to-consumer advertising like every other developed nation in the world. The days of creating a drug market and then selling into it need to come to an end.
Second, reference pricing of pharmaceuticals like Canada and European nations do. Set our prices so they come in line with the rest of the world.
Third, don’t buy the innovation argument from a medical-industrial complex that has over-promised and under-delivered while padding executives pockets. Trust me – American innovation can stand on its own two feet without systematically breaking the financial backs of average American families.
Tags: drug prices > health reform > KFF > Medicare-for-all > universal health care
Our Coast Guard Families Deserve Better.
Posted on | January 16, 2019 | Comments Off on Our Coast Guard Families Deserve Better.

Mike Magee
On January 15, 2019, Admiral Karl Schulz informed 42,000 members of the Coast Guard and their families they would not be receiving their January paychecks because of President Trump’s wall-induced government shutdown. “I recognize the anxiety and uncertainty this situation places on you and your family, and we are working closely with service organizations on your behalf,” he wrote.
This is a long way from February 17, 2005, when Commander Bill Kelly, Captain Jim Thomas, Captain Robert Dash, and Chief Warrant Officer Guy Cashman welcomed me to the Coast Guard Academy to address their executive team on leadership. Since 9/11, we had been working closely together after the release of the book “All Available Boats” which recounted the largest maritime evacuation since Dunkirk, under the direction of our Coast Guard.
The Coast Guard – lifesavers, guardians, warriors, and certainly the most underrated Armed Force in America – is a treasure and a uniquely trained humanitarian force, as prepared for peace as it is for war.
Fourteen years ago, in New London, CT, I emphasized that change was the critical lever defining leadership. Pull it one way and you create a positive leader. Pull it the other and you create a negative leader.
Back then I said, “Negative leaders are short-term thinkers who use fear as a currency to herd people together and move them in whatever direction suites their needs.”
As we have recently witnessed, in the short term, it is a successful strategy, but suffers from a critical weakness, and that is that heightening fear causes people to retrench, reinforcing old beliefs and behaviors, naturally segregating segments of society, reinforcing silos and resisting change.
In the medium and long term, fear holds the population in place, even as the world around them continues to change. This inability to evolve, to stay in step, or to step ahead of a changing world, insures that negative leaders will eventually fail.
In contrast, positive leaders view change as exploration, and lead with vision rather than fear. Their view is long-term and they reach out across the divide. Rather than segregate, they congregate. Rather than build walls, they build islands of common stewardship.
The Coast Guard Academy is an island of common stewardship.
Why should our current level of fear concern us?
Well first, fear is the currency of negative leaders, and they are more likely to emerge and succeed in a fearful environment.
Second, fear undermines trust, and trust is the fabric of a civic society.
Third, fear clearly has short and long term mental health implications.
Fourth, fear accumulates, especially in those who are already fearful. Post 9/11 studies showed clearly that fear biased women and minorities.
And, finally, fear obstructs vision, actively discouraging imagination, innovation and hopefulness. In compromising our wonder and inventiveness, fear fundamentally alters our collective future.
The Coast Guard finds itself in a unique position in today’s world. As a humanitarian force it is both proactive and reactive. Grounded in history, tradition, values and service, it is known and respected by all. At the intersection of two powerful metaphors, it exerts great influence and arouses great expectation from those it serves.
What are those two metaphors? They are water and vessels.
Water representing life, purity, and goodness and vessels with the capacity to transport us to a better place. Water signals revitalization and rebirth. Vessels contain hope and kindness, safety and salvation, equity and justice. At this intersection of water and vessel you will find the future hopes and dreams of not only the Coast Guard and their families, but also the human race.
With the Coast Guard’s help and guidance, we are more likely to find liberty, opportunity, security, civility and democracy on these and other shores.
On 9/11, the Coast Guard reminded us that people are basically good, but they are not perfect. People are basically kind, but when afraid they may act unpredictably. People are basically loving, but when misled respond with hatred and contempt. People are people.
That is why the Coast Guard continues to devote as much time and energy to the preparation for peace as they do for the preparation for war. For our homeland will never be secure if fear has so weakened the fabric of our society that we lose the capacity to be human and humane toward each.
Trump’s political gamesmanship has now ensnared these 9/11 heroes and their families. The Coast Guard deserves better. We all deserve better.
Tags: 9/11 > border security > border walls > homeland security > oast Guard > positive leadership > Trump's government shutdown
Should U.S. Presidential Candidates be Drug Tested?
Posted on | January 14, 2019 | Comments Off on Should U.S. Presidential Candidates be Drug Tested?

Mike Magee
During a nationally televised speech last week on border security, the airwaves lit up. But the discussion was not limited to fact seekers by now well accustomed to counter-checking the President’s deliberate misrepresentations. Joining in were health professionals and addiction experts who literally counted the number of Trump sniffs that became prominent half way through the brief 9 minute teleprompter address.
Sixty (60) was the calculation – enough to revitalize a earlier Newsweek story citing a former NBC staffer’s claim that the president is addicted to snorting crushed Adderall. Arm chair analysts quickly made their own assessments noting that such speculation was consistent with the President’s seeming inability to tell the truth, sometimes erratic behavior, bizarre sleep schedule, and hasty governance by tweet.
Establishing that the President is on a mind-altering amphetamine might at this point be too little too late. Historically presidential succession has been treated as a political rather than a medical process.
Surprisingly, presidential succession was something of an after-thought for the Framers of our Constitution. It was first addressed in 1787 by James Madison with these words, “In case of his [the President’s] removal as aforesaid, death, resignation or inability to discharge the powers or duties of his office, the Vice President shall exercise those powers and duties until another President be chosen, or until the inability of the President be removed.”
It was up to fellow Conventioner, John Dickinson of Delaware, to voice the common concern of the day: “What is the extent of the term ‘inability’ and who is to be the judge of it?” The vagueness of the term “inability” was felt by most future scholars to have been left intentionally vague, as was the role of medical professionals in certifying “inability.”
The nation’s current predicament was voiced by The New Yorker journalist, Evan Osnos, in a 2017 article titled “How Trump Could Get Fired.” He wrote, “unless the President were unconscious, the public could see the use of the amendment as a constitutional coup. Measuring deterioration over time would be difficult in Trump’s case, given that his ‘judgment’ and ‘ability to communicate clearly’ were, in the view of many Americans, impaired before he took office.”
The amendment he refers to is the 25th Amendment to the Constitution, penned by Birch Bayh (D-IN) and ratified on February 10, 1967, following the death of John F. Kennedy. It resolved the issue of Vice Presidential succession to the Presidency and the power of the new President to nominate a new Vice President, pending Congressional approval. It gave the power to declare “inability” to the Vice President and a majority of Cabinet members, with rights of challenge to the President being ousted, who – if he were to challenge – could appeal to Congress to resolve the issue.
What the 25th Amendment did not resolve however was the definition of “inability” and the role and responsibility (if any) of the White House physician or an “expert medical panel.” Bayh for one was opposed to empowering medical leaders in any way other than “consultation as required.” He emphasized that inability was essentially “a political question” and a “professional judgment of the political circumstances existing at the time.”
Essentially, on behalf of his fellow legislators, he was saying, “Not to worry – Congress has this.” But do they under Trump?
Conservative New York Times columnist Ross Douthat set off a firestorm in May, 2017, when he weighed in on Trump inability stating “one needs some basic attributes: a reasonable level of intellectual curiosity, a certain seriousness of purpose, a basic level of managerial competence, a decent attention span, a functional moral compass, a measure of restraint and self-control…Trump is seemingly deficient in them all.”
But other commentators were considerably more restrained, suggesting that impeachment, not the 25th Amendment, is the proper remedy for political malpractice.
Why has the 25th Amendment never been used in a case of active “inability”? The New Yorker’s Osnos says it best. The reason it “has never been used to remove a sitting president is that the inquiry requires assessments of presidential incapacity and mental illness that mental health experts generally want no part of, and politicians are reluctant to engage in.”
Essentially, by the time a President is elected, there is little recourse. As one Princeton professor noted, Mitt Romney in his run for the Presidency “supported legislation mandating drug testing for recipients of federal aid, such as: the unemployed, families in assistance programs — in general, citizens down on their luck or in trouble. Interestingly, none of these politicians has suggested drug tests for executives whose banks benefit from billions in federal aid and bailouts.”
And, he might have added, for any past or present candidate for the Presidency itself. What if mandatory drug testing had been required of all candidates in the 2016 Presidential election? It is quite possible we would have averted our current crisis.
Tags: 25th amendment > presidential inability > presidential succession > role of white house physician
American Health Care’s New Year’s Resolution: Confront The Lie.
Posted on | December 31, 2018 | 1 Comment
Mike Magee

On the last day of a rather disastrous 2018, the Washington Post ran the headline, “Our agents did everything they could.”
The article captured the performance of Kevin McAleenan, head of the U.S. Customs and Border Protection defending his agencies oversight of the death of a second migrant child in the week after Christmas.
On ABC News’s “This Week” his justification read somewhere between ineffectual and reactive. The words: “our agents did everything they could as soon as these children manifested symptoms of illness to save their lives.”
As wicked and depressing as this performance, the words cut deeper still as an indictment of the U.S. Health Care system at large.
In the immediate post WWII period, we never asked the question, “How do we make America and all Americans healthy and productive?” We believed that we could “defeat disease” as we had “defeated the Nazis” – through high-tech, profit-driven, cross-sector collaboration. And that in defeating disease, health would be left in its wake.
Over the half century that followed, practitioners in government, industry and academic medicine discovered each other, and manners of collusion that assured career advancement and steady streams of revenue. In this increasingly organized medical-industrial complex, everyone who cooperated was dealt in – except the patient.
Nearly seven decades into this experiment, this remarkable miscalculation, members of the medical-scientific elite feel more than comfortable suggesting that America’s unhealthy culture is not their problem, and ignore the fact that our’s is the only developed nation that spends more on health care than all other social services (themselves determinants of health) combined.
In 2019, we need to confront the lie that “we did all that we could.” We have not. It is time to return to the original question we ignored, “How do we make America and all Americans healthy?” If we acknowledge the learnings of all other developed nations, we will embrace:
1. Universality: Health coverage and quality accessible health services are a right of citizenship in the United States.
2. Public Administration: Administration of basic health coverage is organized in the most cost-efficient manner possible with central oversight by the government. Incremental steps allowing the option of public sponsored plans to those already insured should be encouraged.
3. Local Control of Delivery: The actual delivery of services to ensure quality and cost effectiveness is provided by health professionals and hospitals at the local and state levels.
4. Health Planning is a Priority: Creating healthy populations is a high priority forour national and state leaders. Working to establish health budgets and priorities, leaders must integrate health services with other social services, advance prevention planning and manage vulnerable populations.
5. Transparency: Providers submit bills. Government ensures payment of bills. Patients focus on wellness or recovery. All essential services (those defined under the ACA) are covered.
Wishing you a happy and healthy New Year!
What Leads To 20,000+ Deaths per Year in American Kids? Autos + Guns = 35%
Posted on | December 20, 2018 | Comments Off on What Leads To 20,000+ Deaths per Year in American Kids? Autos + Guns = 35%
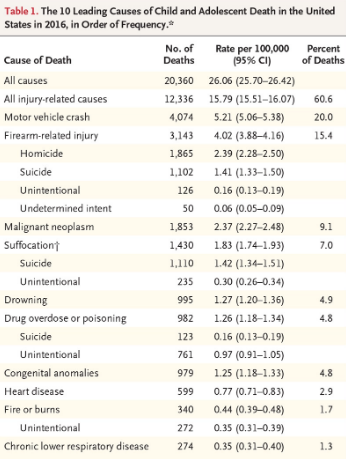
Source: https://www.nejm.org/doi/full/10.1056/NEJMsr1804754?query=featured_home
Commonwealth Report on U.S. Maternal Health Just Released.
Posted on | December 19, 2018 | Comments Off on Commonwealth Report on U.S. Maternal Health Just Released.

The Decoupling of Health from Health Care
Posted on | December 18, 2018 | Comments Off on The Decoupling of Health from Health Care
Mike Magee
“Our health care system’s focus, at every phase of its development, but especially since its expansion and increasing sophistication since World War II, has been on maximizing opportunities for profit and/or career advancement for the players within it.” Code Blue: Inside the Medical Industrial Complex (Grove Atlantic Press, coming in Spring, 2019)
In this week’s Wall Street Journal, Stanford University Hoover Institution fellow, Dr. Scott W. Atlas, reveals, without intention, American health care’s “original sin.”
Atlas is a neuroradiologist and deeply entrenched in the Medical-Industrial Complex, collecting consulting fees for “advising entrepreneurs and companies in the life sciences, medical technology, and health information technology sectors.” His world view is more than adequately reinforced by the Hoover Institution which “seeks to improve the human condition by advancing ideas that promote economic opportunity and prosperity.”
The WSJ piece claims that U.S. health care’s dismal rankings on a global scale are “grossly flawed calculations.” Through Dr. Atlas’s lens, America’s ranking of 32nd of 35 nations in infant mortality is because we over-report compared to comparator nations; and because our mothers indulge in more harmful behaviors; and because America possesses higher rates of “racial and ethnic minorities.”
As for America’s plunging life expectancy rates (ranked 26th for men, and 29th for women), he, without irony, adopts a “Don’t blame us!” posture, pointing instead to “unhealthy lifestyle choices, violence, urbanization, marriage and economic inequality.”
As for treating the diseases that he blames on others, he celebrates America’s “superior results”, and our remarkable access to surgeries, screenings, diagnostics and drugs, without mentioning our remarkable over-consumption, our permissive risk/benefit calculus, our raging opioid epidemic, or our near half-million avoidable deaths a year in unsafe hospitals.
The reader is left with the feeling that we all live in an alternative universe, where health is decoupled from health care, where cause can not be linked to effect, and where a privileged world view comfortably co-exists with remarkable and growing levels of unconscionable inequity.
Dr. Atlas’s essay does little to advance his cause. Rather, it reveals a stubborn committment to the status-quo and adherence to American health care’s “original sin.” In the immediate post WWII period, we never asked the question, “How do we make America and all Americans healthy and productive?” We believed that we could “defeat disease” as we had “defeated the Nazis” – through high-tech, profit-driven, cross-sector collaboration. And that in defeating disease, health would be left in its wake.
Nearly seven decades later, this remarkable miscalculation is so well entrenched that members of the medical-scientific elite feel more than comfortable suggesting that America’s unhealthy culture is not their problem, and ignore the fact that our’s is the only developed nation that spends more on health care that all other social services (themselves determinants of health) combined.
"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
Homegrown Friends
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY

