“Where’s the Beef?” Water as Currency.
Posted on | March 1, 2019 | 3 Comments

Mike Magee
“They want to take your pickup truck. They want to rebuild your home. They want to take away your hamburgers. This is what Stalin dreamt about but never achieved”, screeched former White House aide Sebastian Gorka at the Conservative Political Action Conference this week.
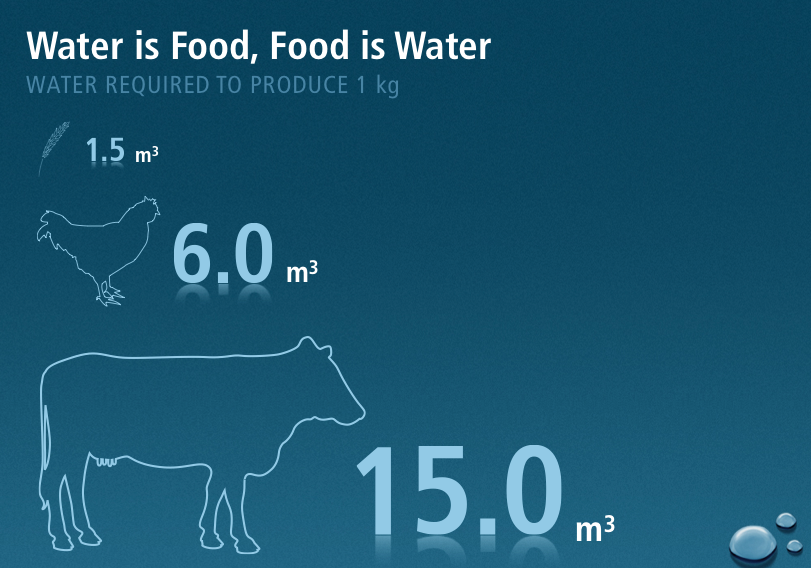
His widely discredited remarks were called out by a range of environmental scientists who laid out the role of American’s dietary habits as contributors to carbon dioxide production and global warming. For me, it recalled the slide above, part of a year long speaking tour I conducted in 2006 in support of the publication of Healthy Waters. The slide demonstrates the relative consumption of water resources to produce 1 kg of grain, versus 1 kg of chicken or beef as food.
Remarkably, we Americans require approximately 3 liters of water a day for survival, but the average America diet (heavy in beef) requires an investment of 3000 liters of water a day.
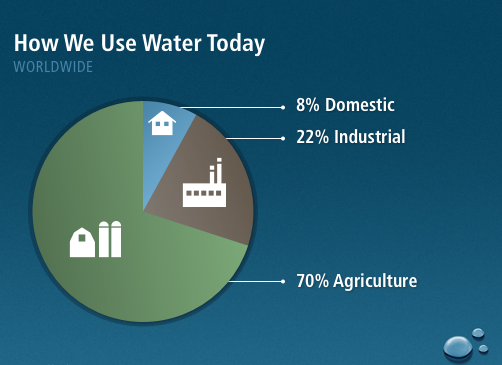
As the slide above from the same presentation illustrated, 70% of our water consumption is in support of our dependence on meat-heavy agriculture in this country.
It’s easy to make the case, for human health reasons alone, to shift in the direction of a plant based diet. What is more easily overlooked is that Americans obsession with meat has threatened in equal measures the planetary patient through its contributions to global warming and water consumption.
The Road to Universal Coverage
Posted on | February 26, 2019 | 1 Comment

Mike Magee
New York Times columnists. Austin Frakt and Aaron Carroll, provided a genuine public service this week in offering an interactive exploration of universal health care. Readers were asked to react to the same questions presented to a bevy of health gurus.
Their 5 “Yes or No” questions were:
1. Do you support automatic enrollment in universal coverage?
2. Do you support ending employer-based private coverage?
3. Do you support replacing individually purchased private coverage, like Affordable Care Act plans or Medicare Advantage?
4. Do you support eliminating premiums and having the system financed exclusively by taxes?
5. Do you support eliminating cost sharing — meaning co-payments, coinsurance, deductibles — for everyone?
Following each vote, you are able to see the % who voted “yes” or “no”. Then there is commentary from health policy notables explaining why they voted the way they did. Spoiler alert – majorities are leaning toward big change.
The national scale is obviously tipping toward idealism and solidarity with significant push back from pragmatists/realists explaining – usually based on taxation/financing – why what logically should be done is just not politically feasible.
What is missing from the piece above, and from many others on the topic, is an obvious truism: Universality is dependent on two co-determinants – mandatory participation and transformational efficiencies.
In short, we can afford health care as a universal right for all only if we share the risk and halt profiteering collusion by the Medical-Industrial Complex.
Consider these two facts:
One in five American dollars now go to health care – we spend close to twice the amount of most other developed nations.
There are 16 health care employees for every one physician in America – and half of these 16 have absolutely no clinical purpose.
Stories of profiteering and financial abuse abound, and I review many of them in Code Blue: Inside The Medical Industrial Complex (Grove Atlantic) due out on May 7, 2019. But let me share just one recent case that illustrates the near racketeering level of absurd waste in our system as described in an investigative ProPublica piece last week.
It seems that nearly all the major health insurers have been secretly greasing the palms of the 100,000 plus U.S. local health insurance brokers to push their products on small and large employers nationwide. Secretly, the brokers have been collecting a 3 to 6% commission on every premium, which for a company of 100 people amounts to a $50,000 plus annual fee. And that’s for the regular plans. If they sell you supplemental plans (for drugs, dental, optical etc.) the commissions are richer – much richer. 40% to 50% to be exact because the benefits often go unused.
Scaling that up, BC/BS’s service of 15 million employees in 5 states generated $816 million in broker bonuses in 2017. And they and other big players like Cigna, United Healthcare and Aetna offer no apologies. To them it’s the price we pay for good, clean competition.
And then there is Morris County, New Jersey, where one fast-talking broker convinced the county’s HR people to switch coverage to Cigna and effectively concealed the administrative charges for the switch – over $800,000. The county is now suing, and consuming more local taxpayer dollars in the process.
A significant and growing contingent of consumer advocates favor big change. Why? Because they realize that crooks thrive in the cracks of complexity. Simplify is their true rallying call, and eliminating steps and “non-real” work is the surest way to finance health care for all.
The Planetary Patient
Posted on | February 12, 2019 | Comments Off on The Planetary Patient

Mike Magee
In 2005, I published a book called Healthy Waters in an attempt to raise environmental health and the deteriorating “planetary patient” as a pressing health care issue. My efforts were only modestly successful.
Chapter 8 in the book was titled “Natural Water Disasters” and summarized the costs in human life and fortune as a result of global warming and environmental degradation.
At the time, no natural disaster had generated more powerful and destructive images than did the tsunami that struck Asia and Africa in December of 2004. That single event, in dramatic fashion, illustrated both the power of water and the vulnerability of coastal and river basin populations.
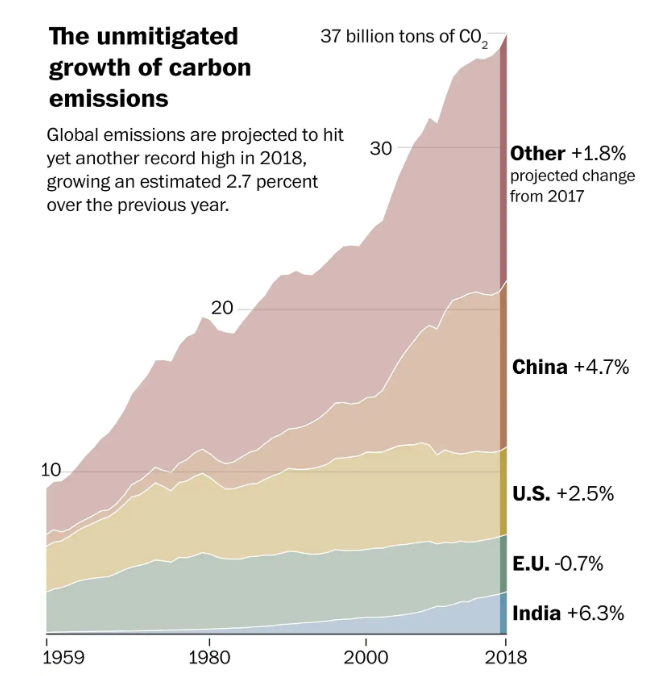
At the time , CO2 levels were 380 parts per million. Now 13 years later, they have risen to 410 ppm. In the age of Trump, manufacturers global carbon emissions have risen from 27 billion tons of CO2 a decade ago to 37 billion tons of CO2 in 2018.
A recent article in the Washington Post on the topic is simply headlined, “We are in trouble.” The Paris Accord had us heading in the right direction with global emissions flat between 2014 and 2016. But in 2017, global emissions rose 1.6% and in 2018 grew 2.7%. In that year, US emissions grew 2.5% while EU emissions declined -1%
Outlining the damage caused by global warming already to our planet would take more room than we have here. In fact, the federal government delivered a 1,700 page congressionally mandated climate impact update to Trump on Thanksgiving, 2018, which left little room for thanks. This came one month after the President’s appearance on 60-minutes where he said, “I don’t know that it’s man-made” (and that the warming trend) “could very well go back.”
Of note in the report: The continental U.S. is 1.8 degrees F. warmer and our seas 9 inches higher than they were 100 years ago.
You don’t have to convince Miami’s Chief Resilience Officer, Susanne Torriente, that there’s a problem. She said, “We don’t debate who caused it. You go outside, the streets are flooded. What are you going to do about it? It’s our reality nowadays. We need to use this best available data so we can start making decisions to start investing in our future. … It shouldn’t be that complicated or that partisan.”
A decade ago, New York Times columnist, Tom Friedman, launched the term “Green New Deal” covering a range of activities he thought might treat the planetary patient’s environmental illness.
The term has now been picked up by Rep. Alexandria Ocasio-Cortez (D-NY) to encompass a range of progressive goals including climate related initiatives. Some claim it will be a litmus test for Democrats, while others predict it will be their demise.
But as the victims of the recent California fires could easily attest, the risk is growing. Back in 2006, I wrote, “Absent preparedness, the losses are complex and considerable, measured in human life and the loss of social, economic and environmental capital. Such disasters are increasingly magnified through human error, can occur out of nowhere, and generate highly uncoordinated responses. Poor and marginalized populations are most often the victims with secondary down cycling of health status a predictable end effect.”
It was true then, and even more so now.
Tags: Carbon levels > clean energy > global warming > trump > US climate Report
“blank”…. FOR ALL.
Posted on | February 11, 2019 | Comments Off on “blank”…. FOR ALL.

Mike Magee
In a Washington Post interview this week, Rep. Donna Shalala, former head of HHS and now a member of Congress from Florida, suggested that democratic reformers focus on universal coverage by whatever means possible. In her view, this includes opening up voluntary access to Medicare (50+), Medicaid (more liberal entry standards), employer based insurance (for employees kids up to age 30), ACA exchanges (with increased subsidies to enhance affordability), and reinforced CHIP.
Without saying it, Shalala and others believe that you don’t have to strong arm people or restrict choice of coverage to make progress. You just need to offer them better options. Her major point, forged by the pragmatism of someone who has been in the battle for a long, long time, is that mandated universal coverage or the “blank…FOR ALL” is what matters – through whatever means possible.
She cites as one example the natural expansion of ACA funded Medicaid which has now been adopted by 37 states (including D.C.), leaving only 14 (out of 33) Republican governor hold out’s.
Despite Trump’s attempts (echoed vigorously on FOX News) to brand efforts to establish “Medicare-for-all” the way Medicare was attacked a half century ago as big government “socialized medicine”, the majority of governors has tacitly acknowledged what Warren Buffett was right when he described the health care status quo as “the tapeworm of American economic competitiveness”.
The decline of state economies reinforced by the burden of weak social service systems, challenged and undermined by a raging opioid epidemic, had caused Republican governors like John Kasich to declare independence when it came to health policy.
Expanded Medicaid celebrated a new approach (within the corridors of defined eligibility) of universality, access, health planning, portability, and integration with other social service programming. Participating governors liked the fact that the program was well funded, that the benefit package was broad (not a sham skimp HSA product), and that they preserved the flexibility within bounds to set the priorities on spending and were allowed to define how best to advance the overall health of their state populations.
The governors learned that centralized administration of a universally available health insurance offering carried distinct cost savings. Specifically, governor guided single payer health delivery under Medicaid came in 22% less costly than privately insured comparators.
Participating governors well understand that the U.S. is the only civilized nation in the world where more is spent on the mechanics of disease fighting than on all social services combined – the very combination of services and supports that help keep a population well.
Given the power and flexibility under Medicaid, they can redeploy essential human health resources. For example, as wildly expensive nursing home use declines, those employees, now mobile are a potentially useful and experienced mobile home services health corps. Given room for experimentation, as they have been under the ACA, governors have applied both innovation and structural remodeling to expand safety, security, and health across multi-generational families.
Despite Trump and McConnell opposition, The Medicaid single payer authority experiment has gone large scale. Under the direction of autonomous state leaders, nearly 80 million have received care of late with extraordinary high satisfaction levels. 34 million of these citizens are children. 2 million new citizens will be ushered into the human race this year through Medicaid prenatal and obstetric coverage. 9 million blind and disabled citizens sleep easier each night thanks to the governors. Nearly a third of the states structure offerings through a managed care approach. All integrate physical and mental health, including addiction services.
Trump and his followers may be intent on creating chaos, promoting regressive legislation, and reimagining reality, but governors in most states are laser focused on solutions – and the more they experience single payer authority and efficiency, and benefit from integrated health planning, the more they and their citizens like it.
So it’s well to remember that it’s not whether you are for or against “Medicare-for-all” that matters. What really matters is that there be central oversight, uniform high standards, careful public health planning, integrated care, and – above all – that comprehensive health insurance be mandatory all-for-one and one “… FOR ALL” .
Dr. Ralph Northam and the Culture of Forgiveness
Posted on | February 6, 2019 | 1 Comment

Mike Magee
Within 24 hours of the airing of Governor Ralph Northam’s 1984 Yearbook page last week, commentators were discussing the implications of his history of racial bias on his performance as a physician.
Second year psychiatry resident Jennifer Adaeze Okwerekwu asked in STAT this week, “Why are we less forgiving of Ralph Northam as a politician than as a doctor?” In the article she says, “To be a healer is to recognize that medicine is a fundamentally human enterprise — we are all flawed and make mistakes, and sometimes these mistakes can cost people their lives.”
As a medical historian and social scientist, I spent more than a few years describing the patient-physician relationship and its important role in a civil society. My bottom line was that doctors are neither saints nor sinners. They are simply human beings like you and I. Their behaviors are impacted by the circumstances and events occurring around them, and by leaders who help shape those realities.
As medical educators, we strive to accept into medical school individuals with the values and qualities required for caring for others without prejudice. Compassion, understanding, tolerance, empathy, and a sense of humanity are but a few. Landmark studies in Philadelphia in 1999, published in Academic Medicine, revealed that we at times fall short of the ideal.
In a 2006 speech at the AMA President’s Forum, I shared the view that, “if all patient-physician relationships were to disappear, stable civil societies would immediately notice the difference. Our populations would be more fearful, less trusting, less tolerant, less connected, less compassionate, less productive, and less committed to the future.”
In the same address, I cautioned the physician leaders assembled that we functioned as part of a society, and were not immune to negative influences. Specifically I said that “negative leaders, who view change with fear and leverage that fear as a currency to control a population in order to reinforce existing and past power silos, who attempt to segregate us one from another to maintain the status quo, deserve our contempt. They not only draw down the reservoir of good will locally and globally, but ensure our medium and long term failure.”
Dr. Adaeze Okwerekwu wisely recognized that, “Health disparities persist when no one corrects mistakes and there’s no opportunity to listen, apologize, or learn. We must face bias head on, or risk repeating our preventable mistakes”
At the same time she states, “I’m thankful medicine is a forgiving profession…My wish was for each doctor or doctor-in-training to listen to feedback, apologize for their mistakes, and learn from their lapses in judgment.”
Reflecting on her chosen profession, she says, “It’s a commitment that allows us room to exercise humility when we make mistakes and change our behavior when it both undermines the humanity of others and the promise to do no harm.”
In a society and a democracy being actively tested, and searching for ways to heal our nation, all Americans would do well to consider her final words:
“To be a healer is to recognize that medicine is a fundamentally human enterprise — we are all flawed and make mistakes, and sometimes these mistakes can cost people their lives. Doctors don’t get ‘canceled’ or forced to resign whenever we err. By being open about these mistakes, we can identify the root causes and work collaboratively to prevent them from causing harm again. When we know better, all of us are able to do better.”
Is Big Change Coming? Jake and Kamala (& Michael and Howard)
Posted on | January 31, 2019 | Comments Off on Is Big Change Coming? Jake and Kamala (& Michael and Howard)

Mike Magee
The decade long battle by Republicans to “repeal and replace” Obamacare is fading slowly into the background. But as this week’s dust up, ignited by CNN’s Jake Tapper’s probing of Presidential candidate Kamala Harris’s views on Medicare expansion revealed, we still have a long ways to go.
By the next morning, two of Harris’s potential opponents were selling fear at wholesale rates. Michael Bloomberg looking for support in New Hampshire declared, “I think we could never afford that. We are talking about trillions of dollars… (that) would bankrupt us for a long time.” Fellow billionaire candidate Howard Schultz added, “That’s not correct. That’s not American.”
Remarkably neither man made the connection between large scale health reform’s potential savings (pegged to save 15% of our $4 trillion annual spend according to health economists) and the thoughtful application of these newly captured resources to all U.S. citizens without discrimination.
Bloomberg’s own 2017 Health System Efficiency Ratings listed the U.S. 50th out of 55, trailed only by Jordan, Columbia, Azerbaijan, Brazil, Russia. Yet he seemed unable to connect addressing waste with future affordability, suggesting Americans must instead accept the way health care is rather than having the courage to pursue how it should be.
Schultz is similarly short sighted. While acknowledging that the manmade opioid epidemic, mental health crises, and income inequality are “systemic problems” and at levels “the likes of which we have not had in a long time”, he failed to connect the cause (a remarkable dysfunctional and inequitable health care system) with these effects.
Today’s greatest risk to continued progress and movement toward universal coverage and rational health planning is sloppy nomenclature. To avoid talking past each other, we need to define the terms of this debate while agreeing on common end points.
“Universal health care” is an end point goal that reinforces the principle that health is a human right rather than a privilege for the most entitled.
“Single payer” is one strategy or tactic for efficiently delivering on the promise of universal coverage. It is often associated with the Canadian health care system. However, the Canadian system is not technically a “single payer” system, in that provision of insurance (set to national standards) and the delivery of the care are the responsibilities of individual provinces, not the national government. A more accurate label for their system would be “Single Oversight/Multi Plan”.
Canada has choice and also maintains a vibrant private health insurance market which covers supplemental health care plans purchased by 90% of citizens to cover roughly 30% of health costs including optical, dental and drugs which are not covered by government plans. Private insurers in the U.S. in the future might play a similar role.
Americans now in sizable majorities have embraced universal and mandated coverage, with choice. There is little need to force citizens with employer based coverage into public options like Medicare or extended Medicaid. Both employers and employees, given time and control, will support this migration on their own if allowed.
The Canadian government’s role is focused on formalized government health planning as well as insurance standards and oversight. The national government also outlaws DTC drug advertising and sets prices annually for all essential drugs. The national government is the guardian of universality and (often overlooked) simplicity. Providers provide. Provincial government pays. Patients concentrate on health and wellness, and are not plagued by insurance gamesmanship and endless bill bickering on the local level.
On the most fundamental level, the U.S. has no such government-directed, national health planning apparatus. Service levels and reimbursement vary widely across an endless array of private and public offerings that have devolved into a “free-for-all.” What we do have are $4 trillion already committed (albeit badly misallocated), a remarkable array of educational institutions, a dedicated network of public health schools and practitioners, an underutilized group of pharmacists anxious to contribute to their full potential, an expanding primary-care army bolstered by nurse practitioners and physician assistants, a testing ground of 50 different states offering the ability to customize various approaches to care within parameters set by the national government, a first-class and highly profitable scientific research and discovery community that could well stand on its own without diverting resources from health planning or patient care, and an enormous number of health system middlemen (16 positions for every one physician) currently involved in non-real work who need to be redirected toward strengthening services that would contribute positively to the social determinants of health—including improvements in nutrition, education, environment, housing, transportation, and safety.
Kamala Harris is right that simple justice demands universal health care for all of our citizens. But the winning argument at the end of the day for fundamentally revamping a broken system that consumes 1 in every 5 American dollars is economic.
The true impact of spiraling health care costs and their secondary effects—including stagnant wages, income inequality, a lack of job mobility, high rates of medical bankruptcy, the closure of rural hospitals, an inability to invest in infrastructure repairs, and our growing national debt – is staggering.
Warren Buffett, a man who knows something about sustainable growth, said recently: “The health care problem is the number-one problem of America and of American business. . . . Medical costs are the tapeworm of American economic competitiveness .”
Trump’s massive tax cut for the richest rich took us from bad to worse. On a percentage basis, the U.S. became the fifth highest debtor nation (as a percentage of GDP) in the world after Japan, Greece, Italy, and Portugal. Predictably, Paul Ryan then resurfaced the notion of cutting health services for the elderly, the poor, the marginalized and discriminated against – to “save Medicare” and address budget deficits that Trump and his allies had exacerbated through recent tax cuts for the wealthy.
For far too long, our leaders have focused on how to make American corporations wealthy. But let us be clear – there is another way. We could have the courage and the will to reapply our more than ample health care assets and reject the status quo. We could vote in change on a large scale. We could elect leaders willing to honestly address a simple, long overdue question: “How do we make Americans healthy?”
Tags: health reform > Howard Schultz > Kamala Harris > Medicare > Medicare-for-all > michael bloomberg
Public Opinion on Health Reform is Moving left for both R’s and D’s.
Posted on | January 24, 2019 | Comments Off on Public Opinion on Health Reform is Moving left for both R’s and D’s.

Mike Magee
If there is a face for a “compassionate capitalist”, many would drop in the wise visage of Warren Buffett who famously declared “Medical costs are the tapeworm of American economic competitiveness.”
Others have stated it differently while agreeing with results of the 2018 Bloomberg health efficiency index placing the U.S. dead last. The problem is systemic and nearly everyone knows it by now. Legendary Princeton health economist Uwe Reinhardt said as much declaring “At international health care conferences, arguing that a certain proposed policy would drive some country’s system closer to the U.S. model usually is the kiss of death.”
If most experts are there, where is the rest of the American public when it comes to a fundamental reboot of our inequitable and wasteful system focused on cure over care and profit over just about everything else?
The quick answer is, “They’re moving left at a pretty fast clip.” That’s the underlying message in a just released poll from the Kaiser Family Foundation. The report states that “Medicare-for-all starts with net favorability rating of +14 percentage points (56% who favor it, minus 42% who oppose it). This jumps to +45 percentage points when people hear the argument that this type of plan would guarantee health insurance as a right for all Americans.”
And this includes growing Republican support. Look at these numbers:
- 77 percent of the public, including most Republican (69%), favor allowing people between the ages of 50 to 64 to buy health insurance through Medicare;
- 75 percent, including most Republicans (64%), favor allowing people who aren’t covered by their employer to buy insurance through their state’s Medicaid program;
- 74 percent, including nearly half of Republicans (47%), favor a national government plan like Medicare that is open to anyone, but also would allow people to keep the coverage they have if they want to; and
- 56 percent, including nearly a quarter of Republicans (23%), favor a national plan called Medicare-for-all in which all Americans would get their insurance through a single government plan.
What are the concerns.
First, cost in the form of higher taxes. Most want to be assured that there will be substantial front end savings with universal coverage. That means simplifying insurance billing so that we no longer have 16 people employed for every physician in America.
Second, efficiency. Americans need to be reassured that universal coverage will not fundamentally undermine basic access to essential services.
Third, lower drug costs. People have grown tired of their politicians protecting well-heeled donors. They want action.
What would break the log jam in currently drugged-up America?
First, outlaw direct-to-consumer advertising like every other developed nation in the world. The days of creating a drug market and then selling into it need to come to an end.
Second, reference pricing of pharmaceuticals like Canada and European nations do. Set our prices so they come in line with the rest of the world.
Third, don’t buy the innovation argument from a medical-industrial complex that has over-promised and under-delivered while padding executives pockets. Trust me – American innovation can stand on its own two feet without systematically breaking the financial backs of average American families.
Tags: drug prices > health reform > KFF > Medicare-for-all > universal health care
"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
Homegrown Friends
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY

