We must be “Declaration of Independence Walking.”
Posted on | November 24, 2019 | 3 Comments

Mike Magee
In the shadow of last week’s Presidential Impeachment hearings, I have been searching for a silver lining. I tell myself it is helpful our Democracy is being stress tested and our Constitutional weaknesses revealed so that we might take corrective actions in the future. I recognize that this is not Trump’s fault alone but our’s as well, having supported a culture rich in celebrity idolatry, and one tolerant of unsustainable levels of inequity. And I acknowledge we live in a land of unbridled capitalism where solidarity and good government are diminished in equal measure.
So I was heartened to see our public servants, several of whom were first generation immigrants, display their competence, professionalism and courage in support of these United States. I want to believe that they, rather than their inquisitors, represent us. I want to believe that any fair-minded viewers could see our taxpayer money well invested in these remarkable women and men, and that we now better understand the art of diplomacy when contrasted with the bare knuckle hooliganism of Guiliani and his band of thugs.
My search for goodness led me back to 2010 and the Annual ADAP Convention at the Georgetown Westin Hotel. ADAP is a non-profit committed to making HIV/AIDS drugs affordable and accessible to all in need. I was honored and pleased to receive the invitation to deliver their keynote address that year from Executive Director, Brandon Macsata, who had been responsible for my original invite nine years earlier. That invite, in turn, was the result of Brandon hearing me address John Kemp’s Disability group the prior year. “Goodness spreads, you see.”, I told myself.
Brandon asked that I reflect on the role of “advanced professionalism” and “enlightened leadership”. To prepare, I relied heavily on a book my son, Michael, had published with the University of Alabama Press in 2004, titled, “Emancipating Pragmatism: emerson, jazz, and experimental writing”. The book derived from his PhD dissertation at the University of Pennsylvania, and extensively delved into the writings of both Ralph Waldo Ellison, author of “The Invisible Man”, and his namesake, Ralph Waldo Emerson.
So what did my son Michael say in his book that was so compelling that I turned to it that day, and return to it today, in the shadow of Trump-led Republican denials?
Page 3: Quoting Emerson, “To interpret Christ, it needs a Christ…to make good the cause of freedom against slavery you must be…Declaration of Independence walking.”
Page 7: On Fake News”, “Ultimately, Emerson came to believe that ‘America’ itself was a kind of text being read, its meaning a matter of collective decision. It followed that one’s linguistic theory, one’s view of how words generate meanings, had potentially large-scale social ramifications. In suggesting that words were ‘million-faced’, Emerson came to realize, he was suggesting that social possibility was remakeable.”
Page 18: On Change and Diversity, “Emerson writes…’the philosophy we want is one of fluxions and mobility’”.
Page 19: On the American Culture and Diversity, “‘Out of the democratic principles set down on paper in the Constitution and the Bill of Rights’, Ellison says, Americans ‘were improvising themselves into a nation, scraping together a conscious culture out of various dialects, idioms, lingos, and methodologies of America’s diverse peoples and regions’”.
Page 24: On the Emerson View of the Evolution of American Language and Culture, “We forget, conveniently sometimes, that the language we speak is not English, although it is based on English. We forget that our language is such a flexible instrument because it has had so many dissonances thrown into it ….from Africa, from Mexico, from Spain, from God knows, everywhere.”
Page 25 and 28: On Creating Our History, “The jazz musician—who, Ellison says, always plays both ‘within and against the group’ — constantly reflects and redefines the ensemble in which he plays. Likewise the ensemble reflects and redefines the larger community to which it belongs….that ‘anticipatory arena where actuality and possibility, past and present, are allowed to collaborate on a history of the future.’”
This has been a momentous week. We have made progress. We are not static, not trapped, not powerless or fixed in place. But there is much left to be done. This should neither surprise nor discourage. On the final page of Michael’s book, he writes, “An emancipated pragmatism happens whenever and wherever a creative mind or community of creative minds engages in democratic symbolic action.”
Democratic – Symbolic – Action. These are more than words. They are a culture of values. Our future is being written now. VOTE.
Tags: citizenship > Declaration of Independence Walking > Democracy > Ellison > Emerson > Impeachment > Michael Magee PhD > Republicans > trump
CODE BLUE: Sequel to The Social Transformation of American Medicine
Posted on | November 22, 2019 | Comments Off on CODE BLUE: Sequel to The Social Transformation of American Medicine
Background: www.codeblue.online
“Code Blue should be in every college Public Health and Health Policy syllabus in 2020!”
In the preface to his 1984 Pulitzer Prize winning book, “The Social Transformation of Medicine”, Princeton sociology professor Paul Starr states, “History does not provide any answers about what should be done… My hope is that this historical analysis may help to illuminate our present predicament even for people of diverse sympathies. I have sought to trace not only the origins of the institutions and policies that are with us today but also the fate of those that failed or were defeated or stunted in their development. I would not be sorry if these analyses of roads not taking serve as a reminder that the past had other possibilities and so do we today.”
Thirty-five years later, medical historian and health economist Mike Magee retraces the same path carrying it into the present and providing an invaluable sequel to Starr’s landmark text. In his acclaimed and comprehensive book, “Code Blue: Inside the Medical Industrial Complex”, Magee not only brings us up-to-date, but also takes us inside a conspiratorial and collusive network of health related corporations and associations committed to profitability over care. As the Kirkus starred review noted, he also “suggests multiple sensible reforms in the realms of medical education, clinical research, publication of medical trials, marketing by pharmaceutical companies, and politically driven interactions within the Medical Industrial Complex.”
Paul Starr’s book changed the way students and professors looked at American health care, questioning whether it was “the best health care in the world.” Mike Magee not only picks up the trail and carries it into the present, but also explains and illustrates how we created the least efficient and effective health care system in the world, and (most importantly) what we should do about it now. Code Blue deserves a prominent location in the modern interdisciplinary college curriculum, and Mike Magee deserves a prominent position on the college speakers’ circuit.
Doctors or Entrepreneurs? The Triple Mission Problem.
Posted on | November 22, 2019 | 2 Comments

Mike Magee
This week’s blockbuster investigative article in Science doesn’t pull punches. Its’ headline: “Investigation reveals widespread double dipping in NIH program to pay off school debt.” The article cites incontrovertible evidence of taxpayer dollar support for student debt loan forgiveness being granted to many clinical investigators (more than half MD’s) who are on for-profit industry payrolls. More than this, rules designed by the NIH itself to curtail double dipping and blatant conflict of interest rules were found to have been broken by the NIH and sponsoring academic institutions in 1/3 of the 182 cases studied.
The history of research fraud and abuse is covered in exquisite detail in “Code Blue: Inside the Medical Industrial Complex.” Spanning eight decades since WWII, academic medical leaders have been able to “have their cake and eat it too” by embracing the concept of a “triple mission” – as clinicians, educators, and researchers all in one. Fraudsters like Arthur Sackler knew well the value of wrapping themselves in academic garment – creating institutes, fraudulent journals, and bogus publications – to create professional CVs and public biographies that defined them as saints when in fact they were sinners.
This mingling of roles is somewhat unique to the Medical Industrial Complex (MIC). Even the Military Industrial Complex recognizes that Boeing is in the job of generating profit; that their paid research promoters are required to register as lobbyists, and that transparency and checks and balances are necessary to challenge outright greed and avarice.
The MIC supply chain, which now controls 1 in every 5 dollars in America, casts a wide net, and includes medical journals (dependent on income from advertising and reprint sales), continuing medical education, voluntary accreditation services, patient advocacy non-profits, and contract research organizations (CROs).
Attempts to bring rule-breakers to heel have repeatedly failed due to “triple mission” comingling. For example, to combat fraud by increasing transparency, in 1997 Congress passed the FDA Modernization Act, requiring that studies for life-saving drugs be registered on a new website, ClinicalTrials.gov, when the studies were initiated. The FDA broadened its criteria for which studies needed to be registered. After four years of experience, it was clear that companies were not rushing to the land of transparency. So, in 2004, the International Committee of Medical Journal Editors, which included editors from JAMA and the New England Journal of Medicine, elected to use their own power to force early disclosure of all studies. Their lever was a declaration that they would no longer publish research papers based on studies that had not first been formally registered on ClinicalTrials.gov.
When the $700 billion pharmaceutical industry threatened to cut off millions of dollars of advertising revenue, the standards-defending editors folded like paper tigers. They knew all too well that drug money, paying not just for ads but for bulk reprints of individual favorable articles, which their reps distributed to doctors, kept these journals alive. Debate and critique played out in critical articles in the journals themselves. For example, a JAMA article in 2009 criticized editors for purposefully vague directives such as “We encourage the registration of all interventional trials.” Authors also shared their analysis of the results of 323 clinical drug trials in the 10 top medical journals in 2008 and found that 176, or 55 percent, were inadequately registered.
In 2007, Congress ramped up oversight with an FDA Amendment Act requiring that all pharmaceutical trials, at any stage in the development process, be registered. It further required that all results, positive or negative, be posted on the site within one year of completion. Five years later, only one in five studies had met their obligations. A review of 8,907 studies that underwent mandatory registration on the government site over a three-year period (2009–2012) found that less than half had reported any results of those trials at all on the site. Five years later, a 2018 investigation revealed that barely three-quarters of the ongoing clinical trial studies had been registered to the site, and journals have not fully embraced the role of policemen for the government’s trial transparency efforts.
In some cases, academic researchers need only lend their name and credibility. For example, a 2011 study that analyzed 630 publications in JAMA, Lancet, the New England Journal of Medicine, Annals of Internal Medicine, Nature Medicine, and PLoS Medicine determined that, based on the voluntary admissions from the 70 percent of authors contacted who agreed to participate in the confidential survey, industry-hired consultants (ghostwriters) were involved in manuscript preparation in 12 percent of the research articles, 6 percent of the review articles, and 5 percent of the editorials—and that is without considering the 30 percent of authors who chose not to participate in the survey.
The numbers on first glance may appear to be small, but they are more than enough to undermine the credibility of these premier medical journals and undermine public trust in the medical evidence presented in these publications.
Any new health care system the nation develops should dismantle artificial protections for academic medicine’s “triple mission”. With 20% of the GDP in tow, medical research, like military research, can more than stand on its own two feet without shielding its behavior behind direct patient care activities. Entrepreneurial medical researchers deserve to be rewarded for their discoveries, but should not be confused with patient care physicians whose stock in trade is compassion, understanding, and partnership, and not dreams of fame and fortune.
Tags: Medical Fraud > medical research > medical-industrial complex > MIC > NIH
“Socialized Medicine” – Can It Work One More Time?
Posted on | November 12, 2019 | 1 Comment
With excerpts from CODE BLUE: Inside the Medical Industrial Complex.
Mike Magee
In an interview that aired this week on Democracy at Work, Professor Richard Wolff asked me about the term “socialized medicine.” My response: Once our nation makes it through the Impeachment hearings, expect the Republican party to pull out the “golden oldies” when it comes to the health care debate.
Just this week, Trump (pro-Russian but not above using Red Scare tactics when necessary) found time to tweet, “These Democratic policy proposals … may go by different names, whether it’s single-payer or the so-called public option, but they’re all based on the totally same terrible idea: They want to raid Medicare to fund a thing called socialism.” At the same time, he continues to work diligently behind the scenes to destroy the Affordable Care Act including authorization of exploitative 364 day plans as “short term” and Medicaid work requirements designed primarily to destroy Medicaid outreach to our most vulnerable citizens.
Not exactly original. Way back in 1944, with Roosevelt elected to an unprecedented fourth term, supporters of a national health insurance program felt their moment had finally arrived. But then Roosevelt died suddenly, and Harry Truman was left to push for universal health insurance, a collective system of shared risk in which the high costs of the sick would be counterbalanced by the low costs of the healthy.
Studies at the time had confirmed and reconfirmed the weaknesses in the American health care system, in particular the fact that the poor and the aged, a rapidly increasing segment of the population, were especially vulnerable. Doctors and hospitals appeared to be inadequate, both in their numbers and in their distribution. Chronic disease was on the rise as soldiers arrived back home, and recent progress in new scientific treatments promoted by academicians of the day suggested that “disease could be eliminated” if only more research were funded.
Truman presented Congress with proposals for comprehensive national health reform. On November 19, 1945, he addressed Congress and had reason to believe his efforts would prevail. After all, weren’t taxpayers already funding the creation of national health plans for our vanquished enemies, Germany and Japan, through the Marshall Plan? Certainly they would support health care for our own citizens at home. But they met stiff resistance from the AMA, which labeled his call for national health insurance and the creation of a national medical board “socialized medicine.” To prevail, the organization teamed up with the Pharmaceuttical Manufacturers Association (now PhRMA) and enlisted the same PR agencies utilized by the tobacco industry to unleash a barrage of blistering warnings. The “Red Scare” worked like a charm leaving Truman to be satisfied with easily neutralized incremental changes.
As the decade wore on, a worsening chronic burden of disease in an increasingly aging American population kept the issue alive. The AMA responded by expanding its state and federal government relations budgets, and by organizing and launching the AMA Political Action Committee (AMPAC) in 1961. In this effort, they were not short on allies. Other provider organizations such as the American Hospital Association, the American Dental Association, and the American Nursing Home Association were equally nervous about allowing government to become their paymaster. Also lining up in opposition were the National Association of Manufacturers, the National Chamber of Commerce, the Pharmaceutical Manufacturers Association, and the Health Insurance Association of America.
To defeat legislation that would become Medicare, the AMA set out to generate thousands of “spontaneous” letters—notably from non-physicians—voicing opposition. Their “trusted spokesperson” recruited in 1961 was a B-movie actor who had already made the transition to corporate spokesman, and who was also the son-in-law of an archconservative physician and Chicago-based AMA bigwig named Loyal Davis. The man in question, Ronald Reagan.
On the 78 LP record distributed by the AMA, in his most reassuring tones, Reagan fanned doctors’ families worst fears saying, “The doctor begins to lose freedom. . . . First you decide that the doctor can have so many patients. They are equally divided among the various doctors by the government. But then doctors aren’t equally divided geographically. So a doctor decides he wants to practice in one town, and the government has to say to him, you can’t live in that town. They already have enough doctors. You have to go someplace else. And from here it’s only a short step to dictating where he will go. . . . All of us can see what happens once you establish the precedent that the government can determine a man’s working place and his working methods, determine his employment. From here it’s a short step to all the rest of socialism, to determining his pay. And pretty soon your son won’t decide, when he’s in school, where he will go or what he will do for a living. He will wait for the government to tell him where he will go to work and what he will do.”
Of course, that was then and this is now. As we speak, strong majorities of American favor universal coverage, health care as a right, and protections for those with pre-existing conditions. In addition, Democratic presidential candidates all support expansion of a public insurance offering as at least an alternative to private health insurance.
Faced with the threat of a single payer, government run system, the AMA has come out in favor of strengthening the Affordable Care Act. They also have quietly resigned from the Medical Industry Complex (MIC) lobbying sham cabal, the Partnership for America’s Health Care Future, stating they were leaving “to devote more time to advocating for these policies that will address current coverage gaps and dysfunction in our healthcare system.”
In the end, we’re fast approaching the point where politicians and medical leaders will have to choose. Do you side with patients or with MIC profiteers?
Tags: ama > Code Blue > Democracy for All > Impeachment > Medicare-for-all > Republican opposition to health reform > Richard Wolff > single payer > Socialized Medicine
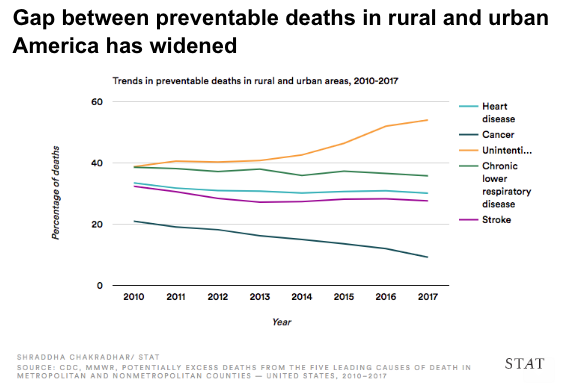
Health Declining in Rural America
Posted on | November 11, 2019 | Comments Off on Health Declining in Rural America
Day of Reckoning on Opioids: Pharmacy Chains
Posted on | November 8, 2019 | 3 Comments
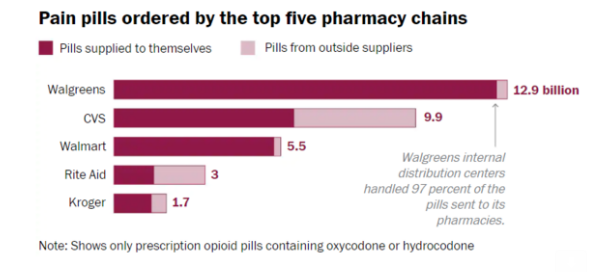
For those responsible for igniting the manmade opioid disaster, a day of reckoning is fast approaching. Of course Pharma is in the cross-hairs – notably Purdue Pharma, Cephalon, J&J, Endo Health Solutions and Actavis. Then come the wholesale drug distributors including AmerisourceBergen Corporation (NYSE:ABC), Cardinal Health, Inc. (NYSE:CAH) and McKesson Corporation (NYSE:MCK). Now giant retail conglomerates like CVS and Walgreen’s are also be caught in the snare.
In this last category, Walgreen’s and CVS are especially vulnerable since their wholesale operations acted as the inside distributor for their retail outlets. Walgreens supplied nearly 100% of their own sales of Oxycontin while CVS supplied more than half of their addictive output. Along the way, as distributors, they carried the liability of ignoring warning signs and government requirements to report unusually large purchases and irregularities in consumption, while bathing in the financial rewards.
For now enablers like the AMA have remained unscathed. They accepted into their Federation a new Pharma-funded pain society which convinced the nation’s doctors that pain was the “5th vital sign”. The AMA also sold its Physician Masterfile Database to data miner IMS Health which allowed the opioid companies to target physicians through prescription profiling who were already sloppy prescribers. AMA sales of the data in 2006 alone brought in $44.5 million.
And let’s not forget a range of bottom feeders like Rudy Giuliani who Purdue Pharma hired to get Bush Administration officials to stand down in their planned prosecution of the company in 2004. Consider the lives that might have been saved had they failed.
But now, the sheer scale of the disaster has caught up with many, if not all of the Medical Industrial Complex offenders. Attorney Mike Moore is leading over 30 state attorney generals in litigation, as he did in the 90’s with tobacco companies. Purdue Pharma is pursuing bankruptcy with states and municipalities pursuing the kind of claw-back on hidden Purdue family money that is reminiscent of the Bernard Madoff affair.
Still and all, it’s pretty shocking that you can literally bring down your entire economy when a greedy profiteering group of health sectors decide to conspire and enable each other. No wonder a sizable portion of the nation is in favor of injecting a healthy dose of “good government” into the health care system. They’re not voting for socialism, they’re voting against conspiracy, collusion, death and the destruction of America’s economy.
How Far Will Republicans Go? If Past Is Prologue…
Posted on | November 7, 2019 | Comments Off on How Far Will Republicans Go? If Past Is Prologue…

Mike Magee
As Jeff Sessions appeals for Donald Trump’s support, and Michael Bloomberg positions to enter the Democratic Primary, with the Iowa caucuses fast approaching, the future of health care, let alone the Republican party, is playing out in full view. The unspoken question, “How far would Republican leaders go to win their own elections? Would they turn on each other? Would they turn on Trump? If past is prologue, this may be a bumpy ride.

Back in 1988, Vice President George Bush was not happy. Since he had announced for the Presidency, all anyone wanted to talk about was his role in Iran Contra. And as polls were revealing problems in Iowa, Bush decided to over rule his advisors and grant an interview to CBS’s career killer, Dan Rather. Why? Because Bush recognized him as a fellow Texan, and therefore a friend. He trusted him. Well, that was a mistake. It hadn’t gone well. The following day, when they asked fellow candidate for the Presidency, Bob Dole, about the performance, he wondered aloud if the vice-president couldn’t handle Rather, what was he going to do about Gorbachev?
Gorge Bush’s people were not amused. Their release, coming right before the Iowa Caucus, read in part, “Iowa Republicans must weigh Bob Dole’s record of cronyism and his history of mean-spiritedness carefully, before they decide whom to support as the Party’s nominee for President.” The release then went on to assert that Bob had “…showed his mean-spirited nature in 1976, when he nearly single-handedly brought the Republican national ticket down to defeat.” Just in case Bob was still self-composed, they insulted his wife as well, noting near the end that Dole’s public statements “…fails to mention that he and his wife are now millionaires, and had an income of $2.19 million from 1982 through 1986.”And for the icing on the cake, there were a few extra reference points including the fancy Watergate apartment complex, the warm weather condominium in Florida, and Elizabeth’s blind trust currently “under federal investigation”. That should do it, they predicted, as they handed the release off to the Iowa Register.
And it did do it. The Register reporter went right to Dole and asked if he believed Bush was behind the release. Dole responded, “Either George Bush is responsible for this kind of campaign…or he’s totally out of control…Maybe he isn’t in charge…Maybe he’s totally out of the loop.” Next stop, Clinton, Iowa, where the vice-president was campaigning. Bush was well-prepared for the question, having been prepped by aides, and armed with an answer that would ensure that Dole’s ire would last well into the New Hampshire primary that was only eight days after Iowa. Was he responsible for the offending release? Bush’s answer: “I don’t endorse it. But I don’t reject it.”
Bush didn’t win a single county in Iowa, but the next day he was in New Hampshire with a new-found focus. He could lose this thing. They took a two-prong approach. First, photo-op’s with the beloved Vice-President, followed by man-on-the-street campaigning across the state, with slugger friend Ted Williams in tow. Second, an attack ad designed to further infuriate an already severely upset Dole. The solution: “The Straddle Ad”. It couldn’t come soon enough. Dole had been working feverishly in the state. and made up 18 points in just three days and was still climbing. The weekend before the election, new poll numbers were released: Dole 32%, Bush 29%.
The Bush camp put in a call to the state’s popular governor, John Sununu, who had been stumping for them. What could he do to help? The Governor had a favor he could call in from the state’s popular Channel 9. A month earlier, he had treated the station to a highly publicized visit by the Vice-President, complete with pictures, hugs, and follow-up notes. They hadn’t forgotten, and at the Governor’s request, they said they’d be happy to free up air time for his new ad. That Sunday afternoon, it aired. The visuals were striking for the time. Dole faced off Dole isssue by issue until the grand finale – taxes. The voice over: “Bob Dole straddles, and he just won’t promise not to raise taxes. And you know what that means.” Driving home the point, the word “Straddles” fades into “Taxes – He can’t say no.”
The strategy more than delivered. That Tuesday, Bush scored a resounding victory with 38% of the vote to Dole’s 29% and Pat Robertson’s 9%. The Southern pastor would soon drop out, but Bob would battle on. The numbers were bad enough that evening, but the final personal affront was still to come. NBC’s Tom Brokaw was reporting the results live in New Hampshire. Bush had been declared the victor that evening, and was live on set with Tom, beaming and happy. Dole was in his hotel room, mic’d up and on camera. But there was no monitor to see Brokaw and Bush. Dole’s earpiece was not live when Brokaw asked Bush if he had anything he’d like to say to Bob? Bush’s congenial reply, “Naw, just wish him well. And meet him in the South.” Bob’s ear piece then comes live with Brokaw’s voice, “Senator? Any message for the Vice-President?” Dole, with eyes, narrow and dark, reminiscent of his mentor Dick Nixon, angrily replies, “Yeah. Stop lying about my record.”
By the end of the primaries, Bush had amassed 68% of the vote to Bob’s 19%. Bush went on to soundly defeat Michael Dukakis, gaining 53% of the popular vote and 79% of the electoral vote. To accomplish this feat, Bush’s handlers employed a secret weapon – a relatively unknown Ohio native, who would later go on to create FOX News for Rupert Murdock. His name was Roger Ailes, who had created the “Senator Straddle Ad.” Ailes encore was the now infamous Willie Horton ad that claimed that the Governor of Massachusetts allowed 1st Degree murders to have weekend passes from prison. Said the ad, “Horton fled, kidnapped a young couple, stabbing the man and repeatedly rapping his girl friend.” The ad ends with a confused looking Dukakis and the statement, “Weekend Prison Passes: Dukakis On Crime”. In commenting on the latest Ailes creation, Bush attack dog Lee Atwater said of Ailes, “He has two speeds: attack and destroy.” As for the creator’s opinion on his own work at the time, he noted, “The only question is whether we depict Willie Horton with a knife in his hand or without it.”
Not surprisingly, when now President Bush returned to the White House, the Democrats, who controlled both houses of Congress, did not meet him with open arms. Bush had inherited a ballooning budget deficit exceeding $150 billion dollars a year. With not so much as an apology, he predictably turned to Bob Dole for help. What is remarkable is that Bob responded, apparently holding no grudge against his life long opponent. After all, this was the guy that Richard Nixon had turned to when he fired Bob as head of the Republican National Committee. This was the guy who Reagan chose over him as vice-president. And this was the guy who insulted his and Elizabeth’s integrity, and labeled him “Senator Straddle” and a tax offender. But at the end of the day, politics was politics, and he was a Republican, and somebody had to keep the country moving. And who knew what things might look like four or eight years from now. You never know.
« go back — keep looking »"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
Homegrown Friends
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY

