What Is The Next Shoe To Drop?
Posted on | May 27, 2020 | 1 Comment

Mike Magee
As Americans haltingly reemerge through the smoldering embers of the Covid-19 blaze, many wonder, “What will be the next shoe to drop?”
Most realize this crisis is far from over. Erratic leadership at the top will be with us at least until the November election. And even with a successful defeat of President Trump, the virus will likely give as good as it gets for at least another 12 to 18 months until a vaccine appears. Economic hardship and displacement will take years more to resolve.
But even now, we are forced to remind ourselves that there are other threats and concerns that demand our attention. To begin with, infectious diseases are only half of our dual disease burden. Chronic diseases from cardiovascular to neurodegenerative to cancer and beyond have not suddenly disappeared. They remain in force, demanding our attention, and taxing our broken health delivery system.
The same kind of misguided policies that created our health care system have also spawned other vulnerabilities. Take for example the recent drama in Sanford, Michigan. On May 21, 2020, the century-old Edenville Dam, stressed by nearly 4 inches of rain, gave way, but not without warning. It was one of over 2000 dams that were deemed by the Association of State Dam Safety Officers to earn an “F”- high-safety threat rating. (95,000 dams earned a slightly better D.)
Global warming has clearly played a role. The last four years have been among the 15 wettest in Michigan’s recorded history. 75% of the earthen dams in the U.S. are privately owned and have an average age of 56 years. They were mostly built to drive mills and generate modest amounts of electricity. Today, most generate no revenue, and repairs go unfunded.
In the case of the Edenville Dam, it is owned by Boyce Hydro Power whose license was revoked by the Federal Energy Regulatory Commission in 2018 for failure to make necessary repairs the company says would have cost 8 million dollars. They say that residential home-owners on the lake created behind the dam share the blame. They went to court to block the company from protectively lowering the lake level for extra security against sudden downpour. They thought it would ruin the view. Those same lakeside residents now look out on a mudflat.
Dams are emblematic of a wide range of neglected infrastructure problems that demand “good government” responses rather than “a thousand points of light” or “beautiful walls.”
In so many ways, the rent has come due. What all Americans need to realize is that a decisive rejection of this administration in November is only the first step. As important will be what follows – the establishment of “good government” driven by national policy that can efficiently deliver strategic planning, prioritization, budgeting, and execution on a national and equitable scale.
Tags: aging infrastructure > COVID-19 > dual burden of disease > health reform > trump > unsafe dams
Covid-19 and The Collapse of the Medical Industrial Complex: Imagining a Brighter Future.
Posted on | May 23, 2020 | 2 Comments

To our surprise, this online lecture explaining the birth of the Medical-Industrial Complex in America, and how it planted the seeds for the current pandemic disaster, maxed out its Zoom capacity within minutes of its offering. That left many of you in the lurch, and for this, we apologize.
But the good news is, we did a real time recording of Dr. Magee’s presentation, and offer it here to you open access, without charge.
As together we mourn all those we have lost, we encourage you to share this presentation with family, friends and colleagues this Memorial Day as together we pursue a brighter future.
Access the Slide Lecture HERE.
Tags: Code Blue > COVID-19 > MedicalIndustrial Complex > MIC > online lecture
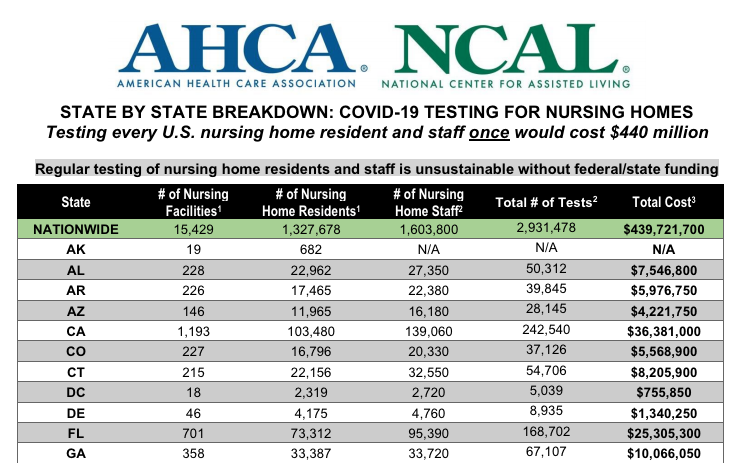
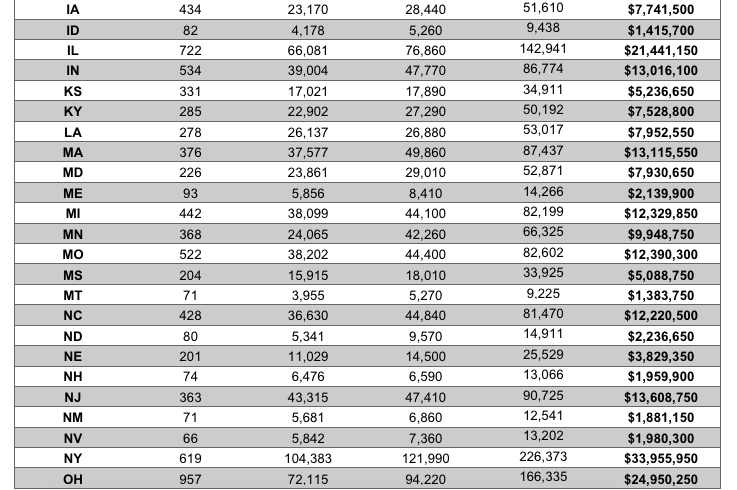
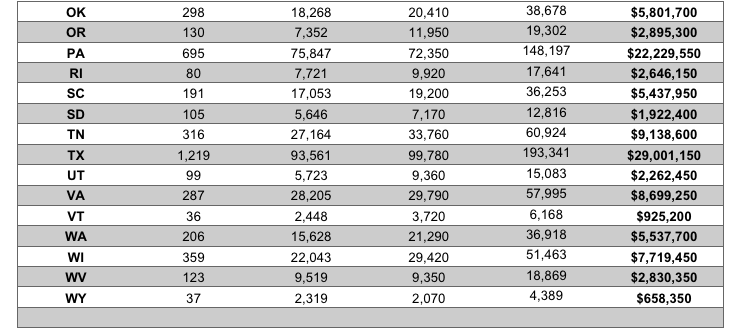
Covid-19 Financial Impact on Nursing Homes
Posted on | May 21, 2020 | Comments Off on Covid-19 Financial Impact on Nursing Homes
“Obamagate” – Why Trump Shouldn’t Go There.
Posted on | May 18, 2020 | Comments Off on “Obamagate” – Why Trump Shouldn’t Go There.

Mike Magee
President Trump’s latest ploy to distract us from his remarkable covid-19 failure, as American deaths approach 100,000, is tossing out the vague term “Obamagate.” He presents the term in the same conspiratorial whisper voice he once used to launch and sustain the “birther campaign.”
It is a mark of understandable desperation that he would mine past territory. Yet, he will likely live to regret drawing attention to this very popular and very competent past-president. The facts are especially damning. If there was ever a pro-science president, it was Barack Obama.
In June of 2009, President Obama first convened his President’s Council of Advisers on Science and Technology (PCAST), and offered this challenge, “So if you guys are so smart, how come you’re still making this (vaccines) with eggs?” At meetings end, the council had its first assignment – Answer this question: “What does the president need to do to prepare for an influenza pandemic?”
5 weeks later, on August 7, 2009, the council delivered a detailed plan. That plan became a 69-page roadmap titled, “Playbook for early response to high-consequence emerging infectious disease threats and biological incidents.”
The new President’s support for science and scientists was given full voice on his 100th day in office. He said, “Science is more essential for our prosperity, our security, our health, our environment, and our quality of life than it has ever been before. I want to be sure that facts are driving scientific decisions — and not the other way around.”
The President provided both time and access to his top science leader. John Holden, a plasma physicist, headed up the committee and carried a title of Assistant to the President that gave him the privilege of direct access and communication. It was not unusual for them to meet several times a week.
The council’s recommendation that a single individual with security experience be assigned to take the lead during a pandemic led to the president’s appointment of John Brennan in 2009. In 2014, Ron Klain, former chief of staff for VP Joe Biden, took over. During this period, Ebola, Swine Flu, and H1N1 were managed without incident.
As the president’s 2nd term drew to an end, Ron Klain wrote, “The next president should put a coordinating unit together before an outbreak begins.” The 69-page playbook was handed over to Trump’s transition team. It went point by point, including:
“Determine whether to implement screening and monitoring measures, or other travel measures within the U.S. or press for measures globally.”
“What are the key services and critical infrastructure that need to come back on line for society to return to normal?”
On January 21, 2017, Trump was inaugurated.
On January 22, 2017, the PCAST website was erased, including all reports.
Over the next two years, no new director of PCAST was appointed, and two-thirds of the staff was let go.
The new PCAST director, appointed in November of 2019, was a professor of meteorology from Oklahoma. Committee members are now primarily from industry.
In December 2019, the Trump administration was informed that covid-19 was breaking out of China.
The committee met on February 3 and 4, 2020. There was no discussion of covid-19.
On March 10, 2020, President Trump remarked, “Just stay calm. It will go away.”
On March 11, 2020, the WHO declared the global outbreak a pandemic.
On May, 11, 2020, Washington Post reporter Phil Rucker asked, “In one of your Mother’s Day tweets, you appeared to accuse President Obama of ‘the biggest political crime in American history, by far’ — those were your words. What crime exactly are you accusing President Obama of committing, and do you believe the Justice Department should prosecute him?” The president stuttered this response, “Uh, Obamagate. It’s been going on for a long time,…some terrible things happened, and it should never be allowed to happen in our country again…You know what the crime is. The crime is very obvious to everybody. All you have to do is read the newspapers, except yours.”
By June 1, 2020, over 100,000 Americans will have officially died from covid-19.
The History of Presidential Inability and What to Do About It.
Posted on | May 8, 2020 | Comments Off on The History of Presidential Inability and What to Do About It.

Mike Magee
As Medical Historian at the President’s College at the University of Hartford, I’ve been asked to explore the 25th Amendment and its’ utility when confronted with Presidential “inability”. During the current crisis, this one hour lecture is offered free of charge and reviews the history of Presidential inability and succession planning from 1787 up to our present crisis. Q&A is encouraged.
Tags: 25th Amendment. Presidential Inability > medical history > U. of Hartford > White House Physician
What A Difference A Year Can Make.
Posted on | May 3, 2020 | 4 Comments

Mike Magee
What a difference a year, and a global pandemic, can make. In this self-enforced pause, there is a great deal of self-reflection going on.
Back in 2019, Michael Bloomberg, looking for support in New Hampshire declared about Medicare-for-all proposals, “I think we could never afford that. We are talking about trillions of dollars… [that] would bankrupt us for a long time.” And fellow billionaire candidate at the time, Howard Schultz added, “That’s not correct. That’s not American.”
Today, with the health care system visibly tilting and scrambling, and policy loyalists and lobbyists for the Medical-Industrial Complex praying for “silver bullets” while searching for “silver linings”, the terra firma beneath their feet is shifting.
At the time though, neither man made the connection between large-scale health reform’s potential savings (pegged to save 15% of our $4 trillion annual spend according to health economists) and the thoughtful application of these newly captured resources to all U.S. citizens without discrimination.
Bloomberg’s own 2017 Health System Efficiency Ratings listed the U.S. 50th out of 55, trailed only by Jordan, Columbia, Azerbaijan, Brazil, Russia. Yet he seemed unable to connect addressing waste with future affordability.
Schultz was similarly short sighted. While acknowledging that the manmade opioid epidemic, mental health crises, and income inequality are “systemic problems” and at levels “the likes of which we have not had in a long time”, he failed to connect the cause (a remarkably dysfunctional and inequitable health care system) with these effects.
“Universal health care” is an end point goal that reinforces the principle that health is a human right rather than a privilege for the most entitled. It is an expression of national solidarity and reflects a shift in our culture. That is to say, it is the exact opposite of what we are experiencing now – a level of disorder and dysfunction that threatens life and limb, paralyzes our economy, and all with no concrete end in sight.
The reality today is identical to what it was one year ago: The U.S. has no government-directed, national health planning apparatus. Service levels and reimbursement vary widely across an endless array of private and public offerings that have devolved into a “free-for-all.” Our profit-driven, scientific research community continues to divert resources from health planning and patient care, and our insurance system harbors an enormous number of health system middlemen profiteers to support “non-real” work (16 positions for every one physician – half with no clinical role).
What we do have are $4 trillion already committed (albeit badly misallocated), a remarkable array of educational institutions, a dedicated network of public health schools and practitioners, under-utilized nurses and pharmacists, and a testing ground of 50 different states. These remarkable, yet undervalued and under appreciated resources, are the true bright spots in this pandemic.
The full impact of spiraling health care costs and their secondary effects—including stagnant wages, income inequality, a lack of job mobility, high rates of medical bankruptcy, the closure of rural hospitals, an inability to invest in infrastructure repairs, and our exploding national debt – remains to be calculated as the covid-19 dust eventually settles.
But let us be clear – there is another way. We could have the courage and the will to reapply our more than ample health care assets and reject this insanely reactive and helter-skelter status quo. We could vote in change on a large scale. We could elect leaders willing to honestly address a simple, long overdue question that is at the very center of this pandemic: “How do we make Americans healthy?”
Tags: Bloomberg > COVID-19 > health care waste > health reform > Howard Schultz > inefficiency > Pandemic
Public Health, The Media, and The Performance of Deborah Birx.
Posted on | April 28, 2020 | 8 Comments

Mike Magee
Imagine there was a time in our living memory when a Washington Post reporter and a woman public health official shared a mutual passion – the health and welfare of Americans.
Imagine this woman was steely in her determination, but shy and refused the spotlight. And imagine that those lined up against her were both powerful and aggressive, and were on record of having attempted – dozens of times – to get her fired.
Imagine now that she woke up one morning, and picked up her Washington Post in the driveway, walked back to the kitchen table, filled her coffee cup, and read the headline, “Heroine Keeps Bad Drug Off Market.”
And as she reads on, “This is the story of how the skepticism and stubbornness of a Government physician prevented what could have been an appalling American tragedy. The story is not one of inspired prophecies nor of dramatic research breakthroughs.”
“She saw her duty in sternly simple terms, and she carried it out, living the while with insinuations that she was a bureaucratic nitpicker, unreasonable – even, she said, stupid. That such attributes could have been ascribed to her is, by her own acknowledgement, not surprising, considering all of the circumstances.”
“What she did was refuse to be hurried into approving an application for a new drug. She regarded its safety as unproven.”
This is not the story of Dr. Deborah Birx. Her’s is a different story. Faced with wild claims of an errant President that hydroxychloroquine showed promise of curing covid-19, she remained self-sidelined, even after studies demonstrated no efficacy and established that cardiac fatalities were an associated risk of the therapy.
Birx is also the government scientist who allowed herself to acquiesce to her embattled President and appear Saturday evening on FOX News, and in response to the host’s question , “Do you think the media in this country has been fair throughout this pandemic?”, responded, “I think the media is very slicey and dicey about how they put sentences together in order to create headlines.”
And she is the doctor who, 12 hour’s later, appeared on Jake Tapper’s CNN Sunday program and was questioned about the President’s suggestion that ingesting or injecting disinfectants might be helpful. Asked “As a doctor, doesn’t that bother you that you have to even spend any time discussing this?”, she defended her bosses remarks as “musings”. And then said, “It bothers me that this is still in the news cycle, because I think we’re missing the bigger pieces of what we need to be doing as an American people to continue to protect one another. As a scientist and a public health official and a researcher, sometimes I worry that we don’t get the information to the American people that they need when we continue to bring up something that was from Thursday night.”
The other Public Health doctor, received the President’s Award for Distinguished Civilian Service on August 7, 1962, in acknowledgement of her strength and personal fortitude which protected thousands of children from thalidomide, and lead to the passage of the Kefauver-Harris Amendment that required drugs be proven to be not only safe, but effective. Her name was Frances Oldham Kelsey, and she worked for the FDA for thirty more years, and died at age 101.
She remained friends for life with Morton Mintz, the Washington Post reporter, who broke the thalidomide story. Their values were well aligned as this salute to him by his colleague, Colman McCarthy, on Morton’s retirement in 1988, suggests.
“Mintz regularly wrote stories after reading thousands of pages of trial transcript, court exhibits and pre- and post-trial proceedings. Were he less a shelf rat and more a show horse, Mintz might be better known. But not better respected. His stories had reach because his commitments had depth.”
Dr. Birx is not Dr. Kelsey. But the Washington Post and New York Times have many reporters who, in their journalistic service to our nation, emulate Morton Mintz, and who must continue to make him proud. He is 98 and lives in Washington, DC.
Tags: coronavirus > COVID-19 > Deborah birx > frances kelsey > morton mintz > thalidomide > washington post
"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
Homegrown Friends
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY

