Open Source and Worth Sharing: A Jesuit Perspective – “Contemplating U.S. Health Care After Covid-19”
Posted on | August 24, 2020 | Comments Off on Open Source and Worth Sharing: A Jesuit Perspective – “Contemplating U.S. Health Care After Covid-19”
“Show Me State” Abandons Trumpian Orbit and Embraces Medicaid Expansion.
Posted on | August 18, 2020 | 4 Comments
Mike Magee
Idaho
Utah
Oklahoma
Nebraska
Maine
…..
(and now) Missouri.
Since 2017, six Republican-led states have buckled under the crippling costs of health care and embraced the ACA offer to subsidize expanded Medicaid coverage for vulnerable populations in their states.
The “Show Me State” showed its defiance and hard-heartedness until their state budget bled bright red in response to mismanagement of the Covid-19 pandemic. The final reversal came in earshot of Trump’s musings to Chris Wallace on FOX about a “health-care plan within two weeks, a full and complete health-care plan” and laughable pledges to “repeal Obamacare” just as 45 million additional Americans became unemployed and uninsured simultaneously.
By 6%, Missourians voted to extend health coverage to an additional 200,000 state dwellers. Those votes came dramatically from former Trump leaning suburbians. Even the state’s rural voters are beginning to get the message, having seen 10 rural hospitals shut their doors in the past few years.
Twelve hold-out states remain – 8 of the 12 from the Old South. That leaves some 2 million vulnerable citizens without coverage that is readily available. Polls in those states show that 2/3rds of their citizens favor Medicaid expansion in opposition to their own governors – and that was before the pandemic. Even in red counties of red states, 1/3 of Republicans are polling in favor of Medicaid expansion.
Democratic politicians like Montana Senate candidate Steve Bullock are running with the news. He’s up on the air promoting state expansion of Medicaid to benefit “rural hospitals all across Montana.”
Who’s next? All eyes are on Florida and its 2.7 million uninsured residents.
Is This Seasonal Flu or Covid-19?
Posted on | August 14, 2020 | 2 Comments

Mike Magee
“Is this seasonal flu or Covid-19?” That’s the question many doctors and patients hope to avoid this fall.
Here are three strategies designed to avoid panic and even greater disruption of individuals lives and malfunction of our already over-stressed health care system:
Strategy 1: Get Your Flu Shot Early.
Approximately 200 million flu vaccine doses have already begun to hit the market in the U.S. This is a 20% increase over last year and presumes an above-normal demand for the preventitive inoculation. AstraZenca has already released its first shipment of their FluMist vaccine after bumping up its original production by 25%.
Strategy 2: Dual Testing for Flu and Covid-19.
Last month the FDA approved a joint COVID-19 and flu test. This potentially will arm health professionals with a tool to avoid the either/or dilemma that faces them just around the corner.“With the authorization of these tests, the FDA is helping address concerns in anticipation of this upcoming flu season during the COVID-19 pandemic, which might be especially worrying for some Americans” said FDA Commissioner Stephen M. Hahn .
Strategy 3: Target vulnerable populations
In early June, with Trump undercutting infectious disease risk at every turn, the CDC gave $140 million to 64 localities to help states prepare for the flu season. By targeting an increase in flu vaccinations for vulnerable populations and increasing access for uninsured, high-risk people, the agency believes it will achieve a multiplying effect – decreasing hospitalizations for both flu and COVID-19.
Experts at the Institute for Health Metrics and Evaluation now predict over 300,000 U.S. deaths from COVID-19 by December accompanied by a 75% increase in hospitalizations over the next 3 months due to Trump’s encouragement of lax policies for containment. Even if defeated in November, Trump is signaling his intention to spend his last two months in office further complicating and undermining a “good government” response to this health and economic catastrophe.
This leaves control mesures in the hands of local leaders, health care professionals and patients. Three things you can do: 1) VOTE, 2) Mask and distance, 3) Get your Flu vaccine early.
The Origin Story of PBM’s.
Posted on | August 13, 2020 | 2 Comments
Mike Magee
Do you know the origin story of PBMs, and why they and their middlemen hold 6 of the top 25 spots in the Fortune 500? Here’s a starter course, excerpted from “CODE BLUE: Inside the Medical Industrial Complex” where the full answer resides.
“When PBMs began, insurers and employers believed that this new entity might contribute to cost control by efficiently processing prescriptions, maintaining approved drug formularies, and holding down prices. But they soon realized that ownership of a PBM by a drug-maker, insurer, or a retail pharmacy giant allowed the owner to coordinate pricing decisions, see competitors’ pricing information, and favor some drugs over others in return for kickback payments, even if the consumer unknowingly was forced to pay more.
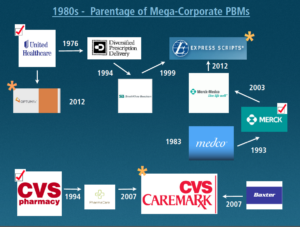
There are now about thirty different PBMs. But three major companies control 78 percent of the PBM market and service 180 million Americans.61 These opportunistic middlemen emerged from three different Medical Industrial Complex (MIC) industry sectors: a physician managed care group, a pharmacy corporation, and a pharmaceutical manufacturing company.
The first one, Diversified Prescription Delivery, was developed in 1988 by UnitedHealthcare, the insurance company that grew out of a physician-run managed care medical group called Charter Med, incorporated in 1974. They were the first to recognize that new information technology would revolutionize the health care industry. Where the WHO owned the ICD-9 diagnosis billing code databases, and the AMA owned the CPT procedure billing code databases, UnitedHealthcare ambitions were far more expansive–to control and mine patient databases themselves. From this perch, they were the first to develop pharmacy drug formularies, hospital admission pre-certification requirements, physician office software that predated electronic medical records, and tight controls on utilization beyond those of other HMO’s at the time.61
The realization that data now was king spread rapidly. A second PBM, PharmaCare, appeared as an offering from CVS in 1994, and in 2007 was renamed CVS-Caremark.62 The third dominant PBM, mail order giant Express Scripts, has a complex parentage. It was formed from the purchase of a SmithKline Beecham’s PBM in 1999 and the addition of Merck-Medco in 2012.63 Five years later, in 2017, Express Scripts reported revenue of over $100 billion compared with Pfizer’s $52 billion of revenue that year.64
Their sphere of influence and market power derives from the fact that approximately 4.5 billion prescriptions are filled in the US each year. Americans’ appetite for legal drugs is close to insatiable. Just under 50 percent of US residents have filled a prescription in the last month, and 10 percent of our population currently takes five or more prescription medications.

Approximately $50 billion is expended each year in the manufacturing of these drugs, which move primarily through three giant wholesale distributors in the US—AmerisourceBergen, Cardinal Health, and McKesson—on their way to the retail pharmacy. Their combined revenue in 2015 was $378 billion for distributing the drugs to 60,000 pharmacy outlets, 63 percent of which are part of large retail chains. By 2017, their combined revenue reached $481 billion.65
PBMs are now the Grand Central Station of the legal trade of drugs and the primary processors of patient and insurance enrollee data. They negotiate the deals for each and every drug with pharmaceutical companies, the placement of those drugs on insurers’ and employers’ tiered insurer formulary drug lists, and the integration and management of utilization and cost strategies with pharmacies, insurers, and hospitals nationwide. Their cutouts and givebacks to both the drug and insurance industries, and negotiations with hospital systems, share the profits and are nontransparent. Nearly everyone is in on the deal—except the patient.”
Tags: AmerisourceBergen > CardinalHealth > CVS Caremark > Express Scripts > health cost > health fraud > health reform > McKesson > MIC > Optum > PBM
A Marshall Plan For America
Posted on | July 30, 2020 | 7 Comments

Mike Magee
Yesterday close to 300 registrants signed up for a webinar sponsored by my Jesuit alma mater, LeMoyne College, titled “The Birth of the Medical Industrial Complex in America, and How Covid-19 Has Made the Case For a National Health Care System”. The college’s motto, “Greatness meets Goodness”, speaks highly of their value system, especially during these challenging times.
During the one hour Zoom presentation, questions flowed in over the chat line which you’ll see reflected in future posts. But the first question asked was, “What do you feel is the most important action step that needs to be taken to start enacting wide-spread change?”
My answer was, “Vote in November.”
I followed that quick response with what I would describe as “A Marshall Plan for America.”
During the presentation, I had shared the fact that, as America’s burgeoning Medical Industrial Complex coalesced in 1950 to beat back President Truman’s plans for a national health care system for our citizens, American taxpayer dollars financed the Marshall Plan construction of national health systems for our two vanquished enemies, Germany and Japan.

In a Rand Corporation post-mortem on nation building some decades later, scholars remarked that, “Nation-building efforts cannot be successful unless adequate attention is paid to the health of the population.”
In the re-build of Germany and Japan under the Marshall Plan, we elected to start with a health plan – in part because we recognized that all other social determinants – justice, housing, nutrition, education, clean air and water, transportation, safety and security – would be enhanced in the process.
We understood that this 1948 infusion of what would today amount to $128 billion would engender trust, improve health and productivity, and process fear and worry which might otherwise undermine the establishment of a civil society and stable democracy.
In answering yesterday’s question, I suggested that we as American citizens essentially face a challenge of similar magnitude.
In rejecting Trump, we are battling the dual scourges of a badly mismanaged pandemic response and the fires of historic and systemic racism. But in addition, we are opening the doors to a cultural and political awakening that could be “A Marshall Plan for America.”
The health care underpinnings of such a plan were driven deep into our cultural soil over a decade ago and have survived relentless attempts to unearth and destroy. These include fundamentals: Health is essential and a universal right. Universal health coverage is necessary to assure population health. All health plans must include comprehensive benefits. Patients with pre-existing conditions must be protected. Our most vulnerable populations are a top priority.
Upon these anchors, and now the sacrifices of over 150,000 Americans dead in part because of Trump’s incompetence, we see revealed the basic “next-step” building blocks of a new deal for America.
Universality: Coverage for all – shared responsibility and risk.
Strategic Planning: Multi-year national health priorities layed out by a truly representative governance body.
Efficiency: Streamline payments, annual negotiated budgets, strict oversight, standardized national billing and payment systems.
Transparency: No DTC advertising. No kickbacks inside PBM’s. No data profiteering. Industry funded academic researchers must register as lobbyists.
Local Control of Delivery: Federal standards with local autonomy. Public insurance is primary. Private insurers are secondary and supplemental.
The unleashing of a Marshall Plan for America could be triggered by the offering of a “public option.” The response of parents of adult children, employees on skimpy employer based plans, newly covid unemployed, underinsured, uninsured and vulnerable will further strengthen our national resolve and advance our evolution towards unification, peace and productivity.
As Trump and Covid have made clear, “a thousand points of light” is no more a substitute for “good government” than it was for our vanquished enemies following World War II. As we did for them then, we must now ask the difficult question “How do we make America, and all Americans healthy?”
And then build out the answer – from the bottom up.
The Cascading Catastrophe of Trump.
Posted on | July 21, 2020 | 1 Comment

Mike Magee
With the ongoing, cascading catastrophe of Trump’s mishandling of COVID-19, it is easy to lose sight that the next pandemic (fueled by global warming, global trade, and human and animal migration) is just around the corner. And we haven’t even begun to nail down the origin story of this one.
Unraveling the transmission trail requires international cooperation. As one expert recently noted, “Origin riddles for other new infectious diseases often took years to solve, and the route to answers has involved wrong turns, surprising twists, technological advances, lawsuits, allegations of cover-ups, and high-level politics.”
What we do know is that there are originators, intermediate hosts, and human super-spreaders….and COVID-19 appears to have begun in China. These are not new insights. We’ve seen this playbook before.
The 2002 Severe Acute Respiratory Syndrome (SARS) rode palm civets to the human hosts.
The 2012 Middle East Respiratory Syndrome (MERS) utilized camals as intermediaries.
The Influenza Pandemic of 2009 traveled through Mexican pigs which had been imported from Europe.
This particular tragedy appears to have begun in Wuhan, China, with the first documented case occurring in December, 2019. The city is the site of the Wuhan Institute of Virology lead by the highly recognized bat virologist Shi-Zheng-Li.
WHO experts will be meeting with China’s experts to share information that has only been released in bits and pieces.
For example, the original working assumption is that this pandemic began in Wuhan’s open seafood market. In January, 2020, there was a small cluster of pneumonias there, and the market was closed and disinfected. But a later study outlined five early cases, four of which had no ties to the market.
The next thrust, fueled in part by the Trump administration, was the pandemic was the result of an inadvertent or purposeful release of the microbe by Shi. Scientists who have now studied the viral genome have uncovered no telltale marks of lab-based engineering.
The lead theory presently is bat-based transmission through an animal intermediary, possibly feral cats, led to the first human infections.
A hostile US government has not served to enhance information exchange. Quite to the contrary. Enlightened leaders are fully supporting the WHO, seeking answers to questions as recently detailed by veteran Science writer Jon Cohen:
1. “Does more epidemiological data exist about the earliest cases than have been made public so far…?”
2. “How aggressively have Chinese researchers looked for SARS-CoV-2 in samples collected before the first known cases in Wuhan?”
3. “Have they looked outside of Wuhan? How far back in time have they probed?”
4. “Can widespread screens be done of bats and other wild animal species thought to be susceptible to SARS-CoV-2 and common in China, including primates, deer, and rodents?”
5. “Can widespread screening of susceptible domesticated animals provide clues to COVID-19’s origin?”
6. “Do stored samples from farmed animals exist?”
7. “Can widespread screening take place of people in China who might come in contact with bats or other wildlife that harbor SARS-CoV-2?”
8. “Do government health reports contain any information about possible COVID-19 cases that predate 1 December 2019, the first confirmed case of SARS-CoV-2 in the scientific literature?”
9. “Are there stored samples from sewage plants in China that can be probed?”
10. “Did Shi’s team ever work with coronaviruses in that lab, and, if so, why?”
Answers to these questions, and many others that affect the future of our nation, await the results of November’s election.
The Supreme Irony of Dr. Trump.
Posted on | July 14, 2020 | 3 Comments

Mike Magee
What a strange irony. Trump decides, full-bravado, to challenge China to a trade war just months before China unwittingly hatches a virulent pandemic that collapses our deeply segmented health care system and our economy simultaneously. And rather than cry “Uncle”, our President then fires the WHO just as their experts are heading to China to attempt to unravel the mystery of covid-19.
And here at home most Americans awaken, forced to acknowledge the absurdity that our case rate and mortality from Covid-19 have made us a pariah worldwide. Our convoluted health system of third-party payers, and the pretzel positions our politicians weave in and out of as they try to justify it, reform it, then un-reform it is defenseless. Congressional loyalists continue to find solace in telling themselves, “Well, we still have the best health care in the world.
In point of fact, we’re not even close to having the best health care in the world. As legendary Princeton health economist Uwe Reinhardt prophetically remarked two years prior to COVID-19, “At international health care conferences, arguing that a certain proposed policy would drive some country’s system closer to the U.S. model usually is the kiss of death.”
It is at times of crises like these that system weaknesses expose themselves. The inability to swiftly and efficiently test a population for COVID-19, share those results, and rationally plan a coordinated and effective response is a reflection of the gross inadequacies of our health care system. So is a leaky and disjointed supply system that can’t manage demand for the basics required to protect health professionals.
In a review of my book, CODE BLUE: Inside the Medical Industrial Complex last year, John Rother, President and CEO of the National Coalition on Health Care wrote, “Code Blue will make you mad, but it will also make you better informed and better able to understand what we need to do as a country to fix it. I can’t think of a more persuasive book on the need for change.”
The need for change that John forecasted not only included matters of justice, planning, and equitable distribution of health care resources, but also the capacity to respond to a global public health disaster of the magnitude of COVID-19.
God Bless Anthony Fauci, and his continued back and forth with Trump, but is our system so fragile that the fate of Americans rests on a single individual having the temerity to speak truth to power in the face of executive incompetence?
A half-century of systematic underfunding of public health, planning and prevention in deference to entrepreneurial scientists in pursuit of profit and patents over patients and families, ends here – in crisis.
We will survive this “Code Blue” calamity, but we need to assure through new leadership and deliberate action that it will never happen again – never.
For now:
- Ignore Trump and Pence.
- Encourage your local leaders and each other.
- Vote with your head, not your heart (or your gut), in the next cycle.
"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
Homegrown Friends
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY

