Lundberg’s Words: “System-shaking, even convulsing.”
Posted on | December 28, 2020 | Comments Off on Lundberg’s Words: “System-shaking, even convulsing.”

Mike Magee
Last week, Medscape’s editor-at-large, George Lundberg, wrote, “In 2017, I published a Medscape column that asked, “How many books will it take?” listing several titles that were intended to provoke repairs or rebuilds. Still nothing happened. Then came COVID, adding massive insult to injury of our already overpriced, overworked, bloated, inefficient, ineffective megalith American procedure-driven medicine.”
Is it possible, as Lundberg suggests, that America has reached a tipping point on health reform?
Exactly two years ago, in the middle of Trump’s caging of immigrant infants and children, the Washington Post ran the headline, “Our agents did everything they could.” The article captured the performance of Kevin McAleenan, head of the U.S. Customs and Border Protection defending his agencies oversight of the death of a second migrant child in the week after Christmas. His exact words: “Our agents did everything they could as soon as these children manifested symptoms of illness to save their lives.”
As wicked and depressing as this performance, these were not isolated actions or even outliers. The Covid spotlight has revealed our weaknesses – especially for the most vulnerable. And the knife cuts deep as an indictment of the U.S. Health Care system at large.
As 2020 draws to an end, Lundberg suggests that we as a nation must finally confront the lie that “we did all that we could.” As yet, we have not.
Our problems are long standing. When I set out to write the 70 year history of the rise of the Medical-Industrial Complex in America, the glaring absence of fundamental national health planning appeared and reappeared year after year. No one across those many years asked the fundamental question, “How do we make America and all Americans healthy?”
In his review of my book, Code Blue, Lundberg writes, “…in order to redesign a system to achieve different results, it would be helpful to understand how the system became the way it is.”
In the reading, you can sense that Dr. Lundberg ultimately found what he was looking for, and admires what he labels “the Herculean task of explaining all this intertwining stuff so that readers can understand how we got here… What Magee does, perhaps better than anyone else in a single location, is name the people, the organizations, the dates, the decisions, the supporters, and the enablers, as well as the victims and the beneficiaries…”
History can go just so far before someone asks, “Where’s the beef?” Dr. Lundberg completes his review by asking, “What to do?”
His answer: “Magee provides a succinct but detailed list of basic steps to reform the medical industrial complex. Five actions involve medical education, seven involve clinical research, five involve publications, and six regard marketing. Incremental, to be sure, but in aggregate, system-shaking, even convulsing.”
I welcome your reviews of Code Blue in the Comments section HERE.
Wishing You a Hopeful and Safe New Year!
Tags: Code Blue > covid > George Lundberg > health reform > JAMA > Medscape > Pandemic
What Do Biden/Harris, Superman and Clean Energy Disruption Have In Common?
Posted on | December 15, 2020 | 4 Comments
Mike Magee
The formal casting of Electoral College votes this week marked the moment that I felt comfortable in removing the Biden/Harris sign from my front lawn. In that moment, with the first Covid vaccines going in and Bill Barr going out, I allowed myself to believe that our new leaders were up to the task of rebuilding our democracy, and making real the ideals of “truth, justice, and the American way.”
That familiar phrase emerged during another epic moment of crisis in our history. It was 1934, in the middle of the Great Depression, when two New York City kids, Jerry Siegel and Joe Shuster, created the comic book super-hero, Superman. America needed a hero then, as we do now – whether they be our nurses and doctors and teachers, or our incoming President and Vice-President.
With the many serious challenges we face at home and around the world, it would be easy to fall into despair and to imagine that our problems are insurmountable. But in truth, there is real progress in the air, and hope for the health of our species and our planet, which has been moving forward under the radar screen.
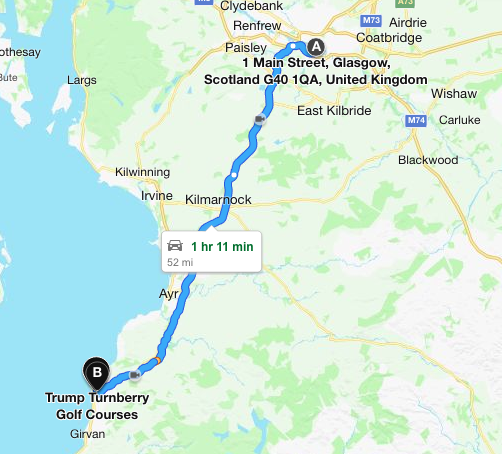
Nowhere is this more evident (though largely hidden from sight) than in our planet’s positioning to address the health and safety fallout of global warming. This week, we celebrated the fifth anniversary of the Paris Agreement, the climate accord signed by 195 nations, which Trump abruptly dismantled four years ago. But President-elect Biden has signaled that his first order on January 20, 2021, will be to rejoin the agreement when the signatories gather in Glasgow, just a short 1 hour 11 minute ride north of the Trump Turnberry Golf Club.
As Trump patronized his fossil fuel funders, and promised that “we’re going to have clean coal and we’re going to have plenty of it,” the oil and gas industry wrote down the value of its assets $170 billion in the first 6 months of 2020.
Acknowledging as much this past week, a cabal of energy investors, with combined assets of $9 trillion, signaled a shift in their strategy with a pledge to harmonize their investments with net-zero carbon emissions by 2050.
Those investors haven’t suddenly “discovered religion.” No. They’re looking at the numbers.
Clean energy options like solar and wind, combined with the latest battery technology, are now 79% cheaper to produce than US coal production. Investors realize that 90% of the new energy capacity generated worldwide in 2020, as reported by the International Energy Agency, has come from clean energy.
Efficiency, profitability, and technology in clean energy are now aligned. The cost of solar panels has dropped 89% in just the last decade, while wind turbines are close behind with a 59% drop in the same time period. The cost of batteries have declined in tandem by 89% resulting in just a two year horizon before electric vehicles reach cost parity with the venerable fossil fuel guzzling internal-combustion engine.
But what about jobs? The news here is even better. Clean energy is currently generating three times as many jobs as fossil fuels. Solar jobs alone are outpacing overall job growth five-fold.
As Trump was fiddling, American cities and states were quietly adjusting their energy investment strategies. Much of the credit goes to former Vice-President Al Gore, whose leadership in this arena has been tireless and earned him a well-deserved share of the 2007 Nobel Peace Prize.
Al Gore will be highly visible as part of the US delegation in November, 2021, when all signators of the Paris Agreement reconvene in Glasgow, just a 1 hour and 11 minute drive north from the Trump Turnberry Golf Course. But the true celebrity at that historic gathering will be infromation technology.
Gore helped Climate Trace in 2019. As their site describes:
“In 2019, a group of nonprofits including US-based WattTime and UK-based Carbon Tracker teamed up to apply for Google.org’s AI Impact Challenge with a proposal to monitor all global power plant emissions from space. Google.org not only selected the project for a $1.7 million grant, but also sent a group of seven skilled data engineering and machine learning Fellows to work alongside WattTime and Carbon Tracker for six months to help bring the initiative to fruition.
After the announcement of the Google.org grant, the teams were surprised to immediately hear from over 50 other organizations and scientists around the world offering to help. So they began systematically investigating: Could mixing and matching innovations from various groups improve global emissions monitoring even further? Among the new collaborators was Vice President Gore, who had long suspected that improved global emissions monitoring through satellites and AI held dramatic potential to accelerate climate progress.”
Gore sees the ability to track real-time atmospheric carbon emissions as a “game-changer.” Combined with efficiency, low cost, and jobs, Gore writes, “This precision tracking will replace the erratic, self-reported and often inaccurate data on which past climate agreements were based.”
With Trump defeated, and a Covid vaccine in hand, and planetary health, racial justice, universal health care, and sane immigration policy cued-up backstage, we have the opportunity to imbue this pledge with pride and substance– truth, justice, and the American way.
Tags: 2020 election > Biden > clean energy > disruption > Harris > Hope > superman > trump
God Bless BioNTech and Pfizer…and Now Let’s Build a First-In-Class National Health Care System.
Posted on | December 12, 2020 | 3 Comments
Mike Magee
As Americans cover-up against second and third waves of Covid-19, Americans once again place their hopes and prayers on a great scientific discovery to snatch us from the flames. The latest miracle cure, the just approved Pfizer vaccine, is highly efficacious and safe, and should provide emergency relief in the days and months ahead. But a single cure does not a health system make.
When Donald Trump expressed his cluelessness—”nobody knew that health care could be so complicated”—before a meeting of state governors in February 2017, he was exposing a pattern of both arrogance and ignorance that remains on full display.
CODE BLUE: Inside the Medical Industrial Complex was published four months later, and accurately predicted that – stressed by a health crisis like Covid-19 – our fundamentally flawed health system would buckle under the pressure. Nearly 300,000 Americans have died, many of them needlessly.
And yet, today we witness a group of Republican Attorneys General appealing to the Supreme Court to dismantle the ACA and the protections it offers to those with pre-existing conditions including Covid-19.
At the very same time, our President-elect has named a group of leading scientists and experts as transition advisers to help take the Biden-Harris COVID plan and convert it into an action blueprint that starts on Jan. 20, 2021.
The Biden coronavirus task force is led by former Surgeon General Dr. Vivek Murthy and Dr. David Kessler. But what if the Supreme Court dismantles the ACA?
We would be left with a convoluted system of third-party payers, and the pretzel positions our politicians weave in and out of as they try to justify it, reform it, then un-reform it. And Republican loyalists would likely continue to find solace in telling themselves, “Well, we still have the best health care in the world.”
In point of fact, we’re not even close to having the best health care in the world. As legendary Princeton health economist Uwe Reinhardt prophetically remarked two years prior to COVID-19, “At international health care conferences, arguing that a certain proposed policy would drive some country’s system closer to the U.S. model usually is the kiss of death.”
It is at times like these that system weaknesses expose themselves. The inability to swiftly and efficiently test a population for COVID-19, share those results, and rationally plan a swift, coordinated, and effective response is a reflection of the gross inadequacies of our health care system. So is a leaky and disjointed supply system that can’t manage demand for cue tips, let alone ventilators and manpower.
In a review of CODE BLUE last year, John Rother, President and CEO of the National Coalition on Health Care wrote, “Code Blue will make you mad, but it will also make you better informed and better able to understand what we need to do as a country to fix it. I can’t think of a more persuasive book on the need for change.”
The need for change that John forecasted not only included matters of justice, planning, and equitable distribution of health care resources, but also the capacity to respond to a global public health event of the magnitude of COVID-19.
How broken must a system be when our nation can’t keep up with nations like South Korea and Italy in testing for the virus? What does our “patchwork response”, variable across states and communities, lacking any private-public planning and coordination, and absent clarity on pricing, access, eligibility and prioritization, and raft with confusion even on what protections are necessary for health care workers collecting samples, tell us about our need for a fundamental restructuring of our health care system?
God Bless Anthony Fauci, but is our system so fragile that the fate of Americans rests on a single individual having the temerity to speak truth to power in the face of executive incompetence? And how are we to reconcile a Presidential veto on testing kits months ago.
A half-century of systematic underfunding of public health, planning and prevention in deference to entrepreneurial scientists in pursuit of profit and patents over patients and families, ends here – in crisis.
God Bless BioNTech’s scientists, Ugur Sahin and his wife Ozlem Tureci, for their discovery, and their partner, Pfizer, for expertise in marketing and worldwide distribution which will be absolutely critical. With their help, we will survive this “Code Blue” calamity.
But we need to assure through new leadership and deliberate action by the Biden/Harris administration that this will never happen again. Scientific bullets are great, but they are no substitute for a first-in-class national health care system which is long overdue.
The Constitution and Your “Right to Health Care” in America
Posted on | December 8, 2020 | 2 Comments
Mike Magee
I’ve been working on a Spring lecture for President’s College at the University of Hartford titled, “The Constitution and Your ‘Right to Health Care’ in America.”
My description reads, “This lecture explores the recent political history and legal controversy surrounding attempts to establish universal health coverage in America. “Is health care a right?” viewed within the context of the Bill of Rights and especially the 9th and 10th Amendments.”
Self-described libertarian-conservative John R. Graham, a health policy analyst in the Trump administration’s HHS, writing on the topic in 2010 stated that, “As a non-lawyer, my understanding is very simple: The Ninth Amendment states that ‘the enumeration in the Constitution, of certain rights, shall not be construed to deny or disparage others retained by the people.’ So, if you claim a ‘right to health care,’ there’s nothing in the Constitution that denies your claim. Indeed, libertarians and conservatives should be more willing to concede a ‘right to health care,’ because once it’s defined as a right, the entire weight of the Constitution comes down against federal (and perhaps even state) control.”
This bit of semantics crash-lands with common sense, as it did in my own state in 1965 when the Supreme Court in a 7 to 2 decision (Griswold v. Connecticut) dismantled an 1873 Comstock Law that prohibited married couples from buying and using contraceptives. Writing for the Court, Justice William O. Douglas declared that “specific guarantees in the Bill of Rights have penumbras, formed by emanations from those guarantees that help give them life and substance.” Though marital privacy was not mentioned in the Bill of Rights, legal analysts have suggested that Douglas was asserting that logic dictated that marital privacy “is one of the values served and protected by the First Amendment through its protection of associational rights, and by the Third, the Fourth, and the Fifth Amendments as well.”
Justice Goldberg concurred at the time, writing: “The language and history of the Ninth Amendment reveal that the Framers of the Constitution believed that there are additional fundamental rights, protected from governmental infringement, which exist alongside those fundamental rights specifically mentioned in the first eight constitutional amendments. . . . To hold that a right so basic and fundamental and so deep-rooted in our society as the right of privacy in marriage may be infringed because that right is not guaranteed in so many words by the first eight amendments to the Constitution is to ignore the Ninth Amendment and to give it no effect whatsoever.”
“Common sense” is what Atul Gawande was mining in his classic 2017 New Yorker article when he went back to his hometown of Athens, Ohio, in the Appalachian foothills, to speak with his now grown-up childhood classmates about “rights” and health care.
Some of his comments drawn from their insights and prejudicies shed light.
“ I had grown up steeped in a set of core Midwestern beliefs: that you can’t get something for nothing, and that you should be reluctant to impose on others and, likewise, to be imposed upon. Here self-reliance is a totemic value.”
“.. A right makes no distinction between the deserving and the undeserving..”
“….‘Frankly, it annoys the crap out of me—they’re nothing but grasshoppers in the system,’ Joe said, recalling the fable about the thriftless grasshopper and the provident ant.”
“… doing all they could to earn a living and pay their taxes—taxes that helped provide free health care for people who did nothing to earn it.”
“Some people see rights as protections provided by government. But others … see rights as protections from government.”
“People don’t think about their water, Tim said, but we can’t live without it. It is not a luxury; it’s a necessity of human existence. An essential function of government, therefore, is to insure that people have clean water. And that’s the way he sees health care. Joe wanted government to step back; Tim wanted government to step up.”
“ The notion of health care as a right struck her as another way of undermining work and responsibility… But Monna, like almost everyone I spoke to, understood perfectly well what Medicare was and was glad to have it…‘We all pay in for that,’ she pointed out, ‘and we all benefit.’… There is genuine reciprocity… To them, Medicare was less about a universal right than about a universal agreement on how much we give and how much we get.”
“… rights are as much about our duties as about our freedoms”
“Trade-offs now have to be considered. And saying that something is a basic right starts to seem the equivalent of saying only, ‘It is very, very important.’”
“…basic rights include physical security, water, shelter, and health care. Meeting these basics is, he maintained, among government’s highest purposes and priorities.”
“‘I think the goal should be security,’ he said of health care. ‘Not just financial security but mental security—knowing that, no matter how bad things get, this shouldn’t be what you worry about.’”
“As he saw it, government existed to provide basic services like trash pickup, a sewer system, roadways, police and fire protection, schools, and health care… these necessities can be provided only through collective effort and shared costs. When people get very different deals on these things, the pact breaks down.”
“The mistake is accepting the line, and its dismal conception of life as a zero-sum proposition. It gives up on the more encompassing possibilities of shared belonging, mutual loyalty, and collective gains.”
“During the next two centuries, we relied on government to establish a system of compulsory public education, infrastructure for everything from running water to the electric grid, and old-age pensions, along with tax systems to pay for it all…Health care has been the cavernous exception.”
“Maintaining the link between health coverage and jobs is growing increasingly difficult, expensive, and self-defeating.”
“Few want the system we have, but many fear losing what we’ve got.”
“What we agree on, broadly, is that the rules should apply to everyone.”
Tags: 10th amendment > 9th amendment > Atul Gawande > health care right > john r. graham > Medicare for all > new yorker magazine > right vs. privilege > universal health reform > US Constitution
My Father Would Be 106 Tomorrow: Why I love him.
Posted on | December 3, 2020 | Comments Off on My Father Would Be 106 Tomorrow: Why I love him.

Mike Magee
My father would be 106 tomorrow. Considering what we have endured as a people, as care givers, as human beings over the past four years, what I wrote about him six years ago bears repeating.
____________________________________________________________________
My father was born on December 5, 1914. Today is his 100th Birthday. And although he died on September 15, 1998, and my mother some three years earlier while caring for him, there is rarely a day that goes by that I do not think of them.
What do I love about my father?
First and foremost, he loved my mother, and everything flowed from that. We kids understood that we were an extension of their love.
I loved his physical presence – that he was big and strong, that he embraced us, held us tight.
I liked that he taught me to whistle, which remains a useful skill.
I was proud that he took care of people as a job, and that the people who he took care of loved him so much.
I liked that every Christmas our dining table was full of baked goods that his patients gave him to thank him for his many kindnesses – giving them time, having open office hours day and night, making house calls when they were scared or worried.
I loved that he was honest, that he didn’t cheat or fudge, that he believed your name had to stand for something.
I loved that he was a gentleman and a gentle man.
I liked that he liked to build things, that he owned tools he rarely got to use, and that he’d get upset because we were always messing with his stuff.
I liked that he liked clothes, especially shoes. He liked to look good, and he wore clothes well.
I liked that he always had lots of change in his pockets.
I liked that he knew the owners of the local stores across the street by their first names.
I liked that he was patriotic and courageous. I learned after his death that he earned a Bronze Star on May 9, 1945. We never saw that medal or ever heard him talk about that day, ever.
I like that he was modest. He didn’t brag. He didn’t have to. I liked that.
I liked that he delegated. He and my mother expected us kids (there were 12 of us) to help teach each other skills like bike riding, and catching a ball, and climbing a tree.
I liked that he took risks, and wanted us to take risks as well – even though a few of those risks turned out to be unwise and too costly.
I liked that he wasn’t perfect – it meant we didn’t have to be perfect, but we did have to try, and we did have to be independent.
I liked that he was often watching in the background, a last stop before disaster, and that his intervention was usually at the direction of our mother.
I loved that the two of them were a team – and that we kids were the players.
I liked that he could take a hit, that he would never fall apart, no matter how bad things were, he would get up the next morning. Our father was reliable, consistent, upright, sturdy, alive.
I thought he was handsome. Others thought so too.
I loved that he was a family man.
I liked that he had a spiritual core – not because of his religious belief system, because his values were secure with or without religion. And not for any punitive conceit – hell rarely made it into our family’s consciousness. No, I liked his spiritual core because it signaled respect for a greater good, a directing hand, the capacity to endure, a reason to try to reach for the stars.
I love my father. He was such a good man. I have tried in some ways to be like him.
(…and, in the midst of this pandemic isolation…)
When I think of him, I always remember one evening, arriving home from college, coming through the door, and being greeted by him. He enveloped me in a big hug that night – tight, long – and kissed me on the cheek, and said my name. He was smiling. His eyes were alive and happy. I can smell him. I can feel his presence.
Tags: caring > doctor > gentle man > leadership > my father > respect > values > William P. Magee Sr.
Thanks and Remembrance: The Polio Volunteers.
Posted on | November 24, 2020 | 6 Comments
 With my sister, Pat – “Polio Volunteer.”
With my sister, Pat – “Polio Volunteer.”
Mike Magee
With vaccines and new leadership now on the horizon, it’s useful to acknowledge that this is not our first pandemic. Of course there was the 1918 flu, but before that – and for many years after – there was polio.
Two years into his first term as President, in 1934, FDR hosted his first “Birthday Ball” and raised one million dollars for his Georgia Warm Springs Foundation – the site he returned to again and again for rehabilitation after contracting the debilitating disease.
He continued the yearly events and four years later in 1938, he broadened the effort creating the National Foundation for Infantile Paralysis (NFIP). To this mix, FDR added two additional resources – great management and celebrity support.
Management came in the form of Basil O’Connor, attorney and close friend of the President. Their friendship predated FDR’s polio and included O’Connor serving as his legal adviser and for a brief period of time as his partner in the practice of law. He would serve loyally in that capacity for more than three decades.
O’Connor’s first order of business was to set up an organizational structure with reach across the country to support services and fundraising. Ultimately, 3100 chapters would be established and $233 million distributed in patient services for children with polio by 1955.
Much of that funding came from a unique idea first presented by radio personality and FDR supporter, Eddie Cantor. Singer, dancer and comedian, he went by the label “Apostle of Pep”, and matched energy level with FDR, stride for stride. At the time Cantor became involved in the Foundation, he had just completed a term as the president of the Screen Actors Guild. In that capacity, he was very familiar with a radio series and accompanying theater newsreel programs titled, “The March of Time”.
Narrated by radio pioneer Fred Smith, and funded by TIME magazine, the program was the first of its kind “dramatized news format” complete with sound effects and music. In January, 1938, Cantor went on his regular radio show and announced the “March of Dimes”, a take-off on the popular newsreel show name. He asked his viewers, young and old, to mail a dime to the President to help beat polio. His many celebrity friends chimed in, amplifying the name and the message, and the “March of Dimes” brand was born. Nearly 3 million dimes arrived at the White House with that first drive, raising 268,000 dollars in change.
Jonas Salk was recruited to the University of Pittsburg in 1947. In 1948, he received a grant from the National Foundation for Infantile Paralysis (NFIP) to identify the various types of polio. But Salk’s goals were much more expansive. He intended to develop the first successful vaccine for the disease and devoted the next seven years to that effort.
Fully funded by the NFIP at $7,500,000, and therefore requiring no need to be distracted by fund raising, Salk initiated a trial on 15,000 children in Allegheny County, Pennsylvania in 1953. The decision to stay close to home vastly simplified the logistics and avoided extra red tape. It didn’t hurt that he also tested himself, his wife and his children or that he achieved startling results on his first try out. Blood drawn from his subjects revealed antibody levels to polio that were 4 to 16 times the levels in non-treated children. These results were reported out in the Journal of the American Medical Association on March 25, 1953.
Following this announcement, which received worldwide attention, Salk took two additional steps that clearly demonstrated both his political and scientific prowess. First he went to Basil O’Connor at the NFIP and secured 100% funding for the largest scientific study that would ever be run in the US. In addition to securing that funding, he enlisted the vast marketing expertise and distribution system of the NFIP.
Secondly, rather than design the trials himself, at a time when scientific competitors were nipping at his heels, Salk enlisted his very popular and highly respected former mentor, Thomas Francis, to design and run the trials. Besides his scientific reputation, Francis had a distinguished record of public service having been the director of the Commission on Influenza for the Army Epidemiologic Board. By 1953, he was a renowned virologist and chair of the epidemiology department at the University of Michigan’s School of Public Health. Once Basil O’Connor with Salk chose Dr. Francis, they carefully created a firewall between themselves and the scientific trials.
Francis was fully aware of the deficiencies in the design. Did every parent clearly read the permission material? Clearly not.Was defining the trial’s purpose “to determine the effectiveness of a vaccine in preventing paralytic poliomyelitis” understating the trial’s experimental nature? What sufficed as a “valid parental signature”? Why were the terms “permission” and “human experiment” found nowhere on the consent form? Was Basil O’Connor’s letter on behalf of the NCIP that accompanied the parental materials and defined their child as having been “selected to take part in this great scientific test” overselling? And did he consciously underplay risk and deliberately transfer liability when he capitalized the words “THE VACCINE WILL BE GIVEN ONLY ON REQUEST OF THE PARENTS” in his letter?
My doctor father received a parcel post in his office in the Spring of 1954. It contained indistinguishable vials of the vaccine and placebo. He used the materials to inject the 2nd graders at our school, including my sister Pat. The event was memorialized in a front page photo in the local Hudson Dispatch of my father, needle in hand, and Pat wincing from the shot, but also proudly displaying her button and card declaring her a “Polio Pioneer”. That was Basil’s idea, as it was to give all the children who participated, including the controls who received no injections, buttons as well. In his view, no one should feel left out of this national public effort to beat the enemy – Polio.
The study remains controversial to this date with two arms – randomized and observed control. The former served the needs of scientists, while the later was felt necessary to maintain public support. In the randomized arm, 2nd graders either received the active vaccine or a placebo, and 1st and 3rd graders were left untreated and served as “controls.” In a second observed control model, all 2nd graders received the vaccine.
The end results were startling and have never been replicated since. Beginning April 26, 1954, within a year’s time, 1.8 million children in 15,000 schools in 44 states were recruited for the experiment. 300,000 health professional volunteers, including my father and the majority of the physicians in the United States, participated without pay. 750,000 of the children – all 2nd graders form public and private schools – were part of a rigorous double blind study.
It was Dr. Francis who stood up on April 12, 1955 at 10:20 AM in Rackham Lecture Hall at the University of Michigan in Ann Arbor and declared in his characteristic direct style, “The vaccine works. It is safe, effective and potent.”
As Crisis Hits, Women in the Lead – While Compensation Lags.
Posted on | November 18, 2020 | Comments Off on As Crisis Hits, Women in the Lead – While Compensation Lags.
Mike Magee
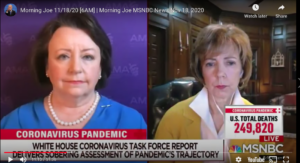
This morning, we witnessed the unusual appearance on network television of two national leaders of the professions of Nursing and Medicine, Dr. Susan Bailey (President, AMA) and Debbie Hatmaker (Chief Nursing Officer, ANA) – both women – appearing in tandem and together, describing the nation’s condition as “very grim” and “quite stark.”
As we struggle to control a second wave of Covid-19, we are reminded once again of the nurses and doctors who place themselves at risk willingly and consistently. And while our attention over the past months has centered on emergency departments and intensive care units, it’s important to remind ourselves that our system of care (where it exists) relies heavily on a primary care base for access to both standard and emergency evaluation and treatment.
In a Medscape physician survey just released today, the financial impact of Covid-19 has been significant. As the report says, “Many physicians offices have closed or have greatly reduced their hours. Hospitals, clinics, and large groups throughout the nation are laying off staff and cutting salaries. Specialties that relied upon elective procedures have lost much or most of their business.”
During the first wave of the pandemic, physician practices reported a 55% decline in revenue and a 60% decrease in patient volume. In March of 2020 alone, 43,000 healthcare workers were laid off nationwide, and nearly 1 in 10 practices closed their doors, at least temporarily. Picking up some of the slack, reimbursable virtual patient visits increased 225%.
The annual Medscape compensation survey was pre-Covid (October 4, 2019 – February 10, 2020), and included over 17,000 surveys in over 30 specialties. In Family Medicine, on average there was a slight $3000 raise (from $231,000 to $234,000) over the prior year. The average time spent per week with patients was similar – 38 hours for men and 35 hours for women Family Physicians. A third of all Family Medicine doctors are now women. Yet the gender gap in salary is striking, with males earning 26% more than women.
The majority of Family Physicians (71%) now work with a team that includes either a Nurse Practitioner (NP) or Physician’s Assistant (PA). Having these teams has increased the profitability of half the practices, and had a neutral effect on 45% of their businesses.
2/3’s of Family Medicine doctors would chose the same career path again, reporting that the three top sources of their job satisfaction are: 1) Gratitude/relationships with patients, 2) Knowing I’m making the world a better place by helping others, 3) Being very good at what I do/ Finding answers, diagnoses.
ANA surveys of nurse satisfaction levels roughly mirror the same determinants. In both professions, these women and men are physically, emotionally, and spiritually exhausted.
What can we do to help them?
- Give Thanks: Expressing gratitude is always welcome. But perhaps the best way to express this in 2020 is to limit gatherings around Thanksgiving, What we don’t need at the moment is super-acceleration of an already bad situation.
- Drop the Political BS. The election is over, and going mask-less in meaningless, and dangerous. Be a good citizen. Wear your mask and a smile.
- Be Patient and Compliant. We’ve got vaccines on the way. But we have a few months to go. When they arrive, get vaccinated without delay.
Tags: covid > family medicine > gender dicrimination in pay > Pandemic > physician compensation > primary health care > Thankgiving > women leaders in health care
"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
Homegrown Friends
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY

