25th Amendment Was Openly Discussed Over Three Years Ago.
Posted on | January 7, 2021 | 3 Comments
Mike Magee
Three years ago, I taught a fully subscribed course at the Presidents College at the University of Hartford on the 25th Amendment. My exploration that year was triggered by a series of articles initiated by New York Times conservative columnist, Ross Douthat.
On May 16, 2017 he wrote “The 25th Amendment Solution for Removing Trump.” I will not summarize the entire course here but would like to accomplish three things:
- Reinforce the fact that the American public was adequately warned (3 1/2 years ago) of the risk that reached full fruition yesterday – but choose not to act.
- Douthat’s piece triggered a journalistic debate which I summarize below with four slides drawn from my lectures.
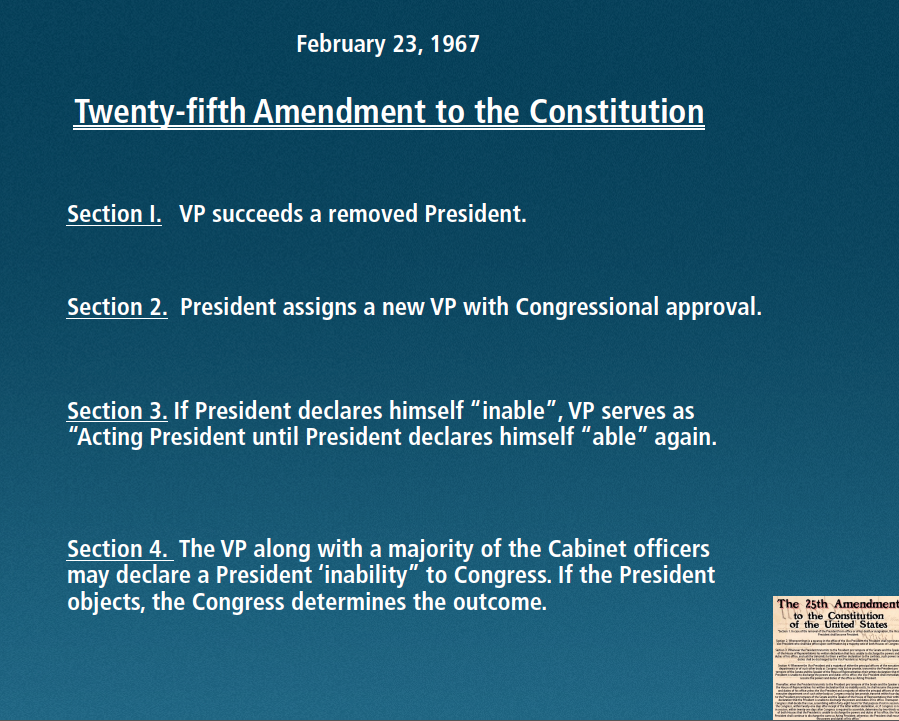
- Were Pence and the cabinet to activate the 25th Amendment, as it is written, Trump would have the right to appeal “his inability”, forcing the Congress to decide whether there was cause to remove the President. With 13 days in his term remaining, procedural timing may preclude the use of this instrument.
Here are the slides:

In 2017, Scott Bomboy, chief of the National Constitution Center, wrote:
“Section 4 is the most controversial part of the 25th Amendment: It allows the Vice President and either the Cabinet, or a body approved ‘by law’ formed by Congress, to jointly agree that ‘the President is unable to discharge the powers and duties of his office.’ This clause was designed to deal with a situation where an incapacitated President couldn’t tell Congress that the Vice President needed to act as President.”
“It also allows the President to protest such a decision, and for two-thirds of Congress to decide in the end if the President is unable to serve due to a condition perceived by the Vice President, and either the Cabinet or a body approved by Congress. So the Cabinet, on its own, can’t block a President from using his or her powers if the President objects in writing. Congress would settle that dispute and the Vice President is the key actor in the process.”
“On our Interactive Constitution website, scholars Brian C. Kalt and David Pozen explain the problematic process if the Vice President and the Cabinet agree the President can’t serve.”
- “If this group declares a President ‘unable to discharge the powers and duties of his office,’ the Vice President immediately becomes Acting President.
- If and when the President pronounces himself able, the deciding group has four days to disagree.
- If it does not, the President retakes his powers.
- But if it does, the Vice President keeps control while Congress quickly meets and makes a decision…
- The Vice President continues acting as President only if two-thirds majorities of both chambers agree that the President is unable to serve.”
There Is No Safe Haven for Patients in the Privatized U.S. Health Care System.
Posted on | January 6, 2021 | 1 Comment
Mike Magee
TIME correspondent Karl Vick, in an article titled “What Happens When Amazon Takes on Health Care”, in February, 2018, wrote: “The U.S. health care system is the antithesis of Silicon Valley.” But is it really?
Vick was referring then to the formation of a new, as yet unnamed non-profit joint venture between Jeff Bezos (Amazon). Warren Buffett (Berkshire Hathaway), and Jamie Dimon (JP Morgan Chase) The triad was joining ranks, they said, to finally bring efficiency and quality to American health care. It would be another nine months before they could settle on a name for the venture – Haven (as in safe haven for their 1.3 million combined employees).
The very public collapse of Haven this week left it unclear whether they were public-spirited crusaders or simply predatory investors in one of the most profitable segments of our national economy.
Analysts have wasted no time piling on. As one said, “Haven had a rocky three years, running up against vague marching orders, a lack of direction, and obstacles inherent to the healthcare landscape.” Another analyst added, this “is a reminder that the U.S. healthcare sector is incredibly resistant to makeovers…”
Insiders pointed to an absence of organizational cohesiveness. All three partners were also pursuing independent ventures in the health care space, and were continually running into proprietary roadblocks.
Amazon, in particular, had its own agenda. Their wearable health tracker, Amazon Halo, augmented by Alexa features, was now joined by virtual and in-person Amazon Care clinics for its own employees. Those employees have access to premium priced prescription drugs after the company purchased PillPack for $753 million in June, 2018.
Other analysts noted a lack of momentum. The first market forays – like their new no-deductible insurance policy – was slow to come and not overwhelmingly embraced by the 30,000 JP Morgan employees. There were also rumors that Amazon in particular was about to pull its financial support.
And yet, it is useful to ask why none of the Triad seem to have regrets.
Jamie Dimon said, “Haven worked best as an incubator of ideas, a place to pilot, test and learn—and a way to share best practices across our companies. Our learnings have been invaluable.”
Warren Buffett said previously, that this was a “a first step in what is bound to be a long journey.“
And a Bezos spokesperson noted, “The venture’s backers found Haven was a good venue to test new ideas and best practices that could be better implemented individually.”
With the election of Rev. Raphael Warnock and Jon Ossoff in Georgia, and the shift of Senate control to the Democrats, will health services continue to be an investment darling?
McKinsey & Company this week offered a qualified yes in a report titled, “The future of healthcare: Value creation through next-generation business models.”
With a straight face, they begin: “The healthcare industry in the United States has experienced steady growth over the past decade while simultaneously promoting quality, efficiency, and access to care.”
But in their next breath comes a yellow caution: “The next three years are expected to be less positive for the economics of the healthcare industry, as profit pools are more likely to be flat.”
Where does McKinsey & Company see profit? They flag information technology, telehealth, and virtual services and delivery as opportunity areas saying, “In the provider vertical, the rapid acceleration in the use of telehealth and other virtual care options spurred by COVID-19 could continue. Growth is expected across a range of sub-segments in the services and technology vertical, as specialized players are able to provide services at scale (for example, software and platforms and data and analytics).”
That should make the Triad smile, but cause patients to shudder.
Tags: amazon > Berkshire Hathaway > Buffett > Dimon > Haven > health reform > JP Morgan Chase > McKinsey
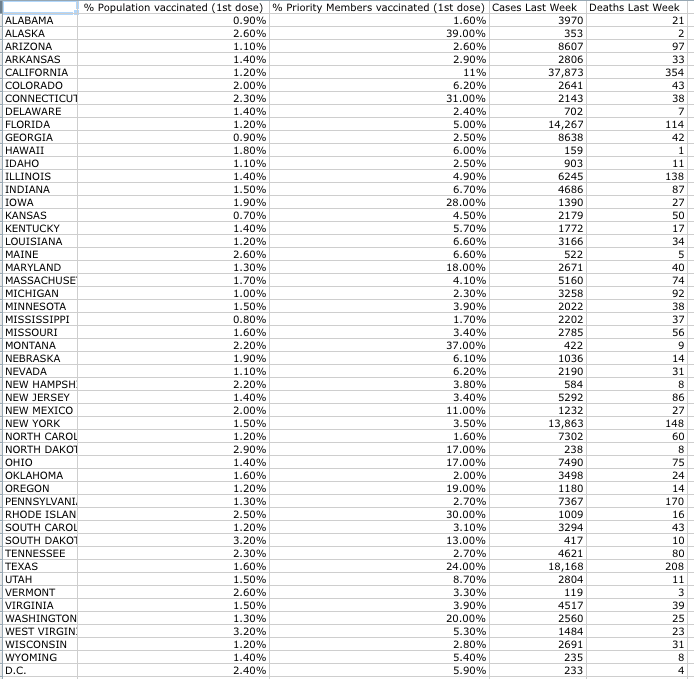
How Is Your State Doing With The Covid Vaccine?
Posted on | January 6, 2021 | Comments Off on How Is Your State Doing With The Covid Vaccine?
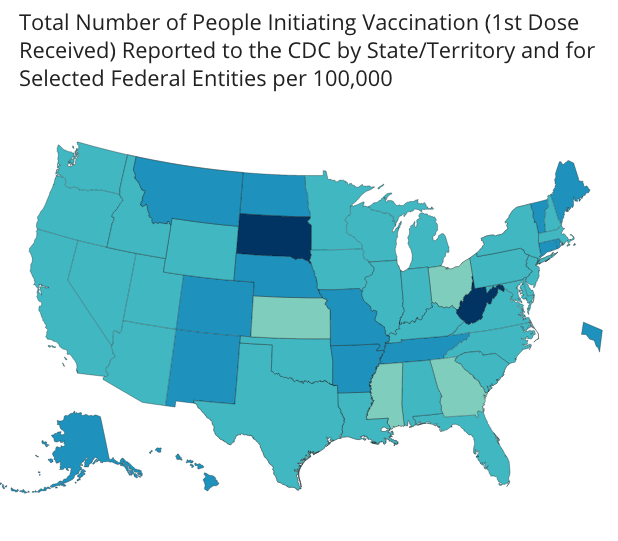
CDC Interactive State Covid Vaccine Map.
Posted on | January 2, 2021 | Comments Off on CDC Interactive State Covid Vaccine Map.
First Post of 2021 – The Pledge and Allegiance.
Posted on | January 1, 2021 | Comments Off on First Post of 2021 – The Pledge and Allegiance.
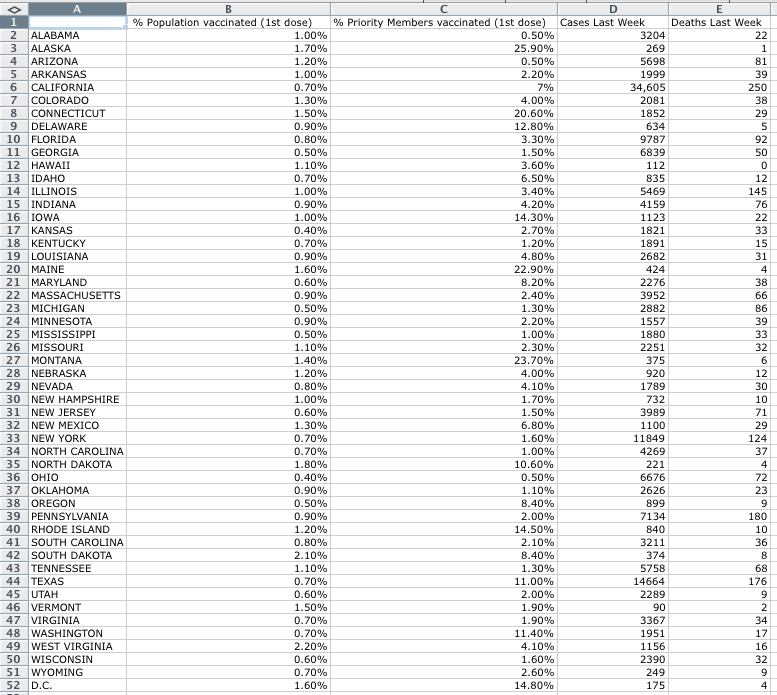
Data Source – Washington Post
Mike Magee
Our new year has arrived. And Covid has more than confirmed the central tenet of “Code Blue” – there is no national health system in America, and little evidence of one “indivisible” nation. Rather we rely on a profit-driven Medical Industrial Complex that is committed to integrating its various guilds and their government relations strategies to maintain and extend financial control.
That is the reality in 2021. The historic conceit – defeat disease, and health will be left in its wake. According to this myth, there is no need for national planning or an integrated public health infrastructure. The silver bullets of discovery and innovation will rescue us “just in time.” That is our silver lining.
“Code Blue” laid out how we got here, and how we might confront and correct it. But in the meantime, Covid appeared, and here we are. Where is that exactly?
Well, we have multiple highly effective vaccinations, but limited capacity to effectively vaccinate our citizens en masse to avoid further disaster. Azar’s promise of 100 million doses by year end, first shrunk to 40 million, then 20 million, but ended the year as only 3 million injections (and that’s a first installment on a double-dose regimen).
Trump washed his hands of the whole mess some time ago. No sense crying over spilt milk, or giving him a moment more of our time. Azar’s team will soon be gone, too. But they’ve already placed the onus on the states – transferring responsibility without funding.
Theoretically, Biden’s team will help a bit, but the reality is rather stark:
- There is no integrated national plan to address this deadly pandemic that has no geographic boundaries in these disunited United States.
- You cannot build public health infrastructure overnight. It takes people, and talent, and money, and data, and systems, and a lot of hard work.
Most of us will survive this calamity of course. We will track the numbers above – comparing one state’s performance to another – tapping into our competitive spirit once again to find the energy to overcome the chaos we’ve inflicted on our own citizens.
But the reality is, as a nation, we need to grow up fast. We need to address our historic inequities, redistribute our wealth among our citizens, explore the meaning of forward planning, sharing and solidarity, and reject cruel and predatory profiteering.
To conquer Covid and heal our nation, even the most cynical of us increasingly realize that we must now create a national and universal health plan. It is the equalizer, the mobilizer, and the stabilizer that is missing and essential. Without it, there will never be “one nation, under God, indivisible, with liberty and justice for all.”
Last Post of 2020: Making Sense of the 70 Million Trump Voters.
Posted on | December 30, 2020 | 4 Comments
Mike Magee
On this final day of 2020, I continue to struggle with this 70 million Trump voter issue.
On the surface, it feels like a broad recrimination of the goodness and intelligence of nearly half of American voters – rendering us “unexceptional” at best.
Even if you grant targeted voters against abortion, or for state’s rights, or concerned about budget deficits, this requires that we accept a remarkable reliance on situational ethics: that you could accept evil, degeneracy, selfishness, and cruelty in a clearly unstable leader if you were able to get what you wanted in the bargain.
While there may be elements of truth in that, I think it’s too simple an explanation. There are other contributors.
We are a consumer society (aka greedy).
We are an individualistic society (aka no tradition of solidarity).
We are a gullible society (aka naive enough to embrace fantasies).
We are an entertainment society (aka easily distractible).
We are a young society (aka immature and quick to discard our elders).
We are Americans (aka vulnerable to someone exactly of the size and dimensions and character of Trump).
The good news, as we enter 2021, is – we are other things as well – innovative, creative, energetic, mostly immigrants, hopeful, and loving (sometimes).
This time around, good conquered evil – barely.
Now we must demonstrate that we know how to use the power to move the needle in favor of our better selves.
How do we make America healthy – in body, mind, and spirit?
That is the question for 2021.
Truth and Trust in 2021.
Posted on | December 29, 2020 | 2 Comments
Mike Magee
Exactly three years ago, veteran Health Policy expert, James A. Morone, Ph.D., made an interesting argument for single payer health care in the NEJM. In proposing a sweeping change that would directly address “the American patchwork”, assert “the norms of communal decency”, promote planning and efficiency, and empower “a righteous band of reformers, deeply committed to a cause, pushing against all odds”, he did not sidestep higher taxes on the rich.
Rather he sold into them, presenting high taxes on the rich in return for universal health coverage as “on a short list of available policies designed to push back on inequality.”
His argument boiled down to the fact that a central element of the national crisis we called “Trump” was populist anger grounded in remarkable income inequality. In roughly a half-century, our separation between rich and poor which used to mirror France and Japan, now aligns with Mexico and Brazil.
Three years later, with Covid ravaging us unabated, we’re a mess, and our citizens are pretty fed up. And why shouldn’t they be? Our top 1% controls roughly 40% of all wealth, while the bottom 90% manages a paltry 23%. If you’re a white family in America, you were born lucky. On average, your family is about 10 times as wealthy as your black family counterpart.
Back in December of 2017, Morone reminded us that major policy changes can, and have, flipped on a dime in the past. As he wrote then, “Disruptive populism ended past American gilded ages, and it shows signs of challenging the current one.” With better health delivery, and more equality and social justice, we might also redirect the course of American politics and American politicians.
In the same issue of NEJM, Henry J. Aaron, Ph.D., explored a different road to reform, raising legitimate concerns about the unintended consequences of disrupting existing insurance holders, and arguing for a more cautious incremental approach including extending availability of Medicare and Medicaid to others, and shoring up ACA exchanges. He wondered then how far and how fast Americans were willing to go?
That same week, New York Times columnist, Thomas Friedman, presciently shared his view. He didn’t pull punches when he accused Trump of intentionally undermining the two critical pillars of American society, truth and trust. And here we are today.
Interestingly, in the careful analysis of these two health policy experts above, both identified an embattled and epic American struggle over how to topple the health care status-quo, a Medical-Industrial Complex controlled and directed by members of the 1%, and a debate that currently hangs on whether we – the citizens – are able to discern fact from fiction.
The key question for health reform and for the future of America: Do we trust a government “of, by, and for the people” to assure that each of its citizens has the right to “life, liberty, and the pursuit of happiness?”
Trump is all but gone -rejected, dejected, marginalized and soon-to-be ignored. It is now on us. If a majority of Americans can move to “yes” on truth and trust, we will find a way to embrace each other equally through health reform. And the quality and durability of that embrace will be determined by these Code Blue principles:
1. Universality: Comprehensive health coverage is a right of citizenship.
2. Public Administration: Administration of basic health coverage is organized in the most cost-efficient manner possible with central oversight by the government.
3. Local Control of Delivery: The actual delivery of services is provided by health professionals and hospitals at the local and state levels.
4. National Health Planning and Coordination is a Priority: Creating healthy populations is a high priority on the federal and state levels. (Covid disaster – never again!)
5. Transparency: Providers submit bills. Government ensures payment of bills. Patients focus on wellness or recovery.
2021 is the year to do right by each other and take care of each other!
Tags: caring and compassion > health reform > health right > income disparity > trump > trust > truth
"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
Homegrown Friends
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY


{kind=link}