Mass Vaccination – We’ve Been There Before.
Posted on | January 30, 2021 | Comments Off on Mass Vaccination – We’ve Been There Before.

Mike Magee
Children of this era, decades from now, will recall a pandemic and their experiences with vaccines, in the same manner as citizens of my age recall the polio vaccine campaigns in the 1950’s.
While my generation was less informed on the science than our counterparts today, we had three advantages:
- National administrative leadership of vaccines and their distribution.
- A focus on mass immunization rather than preferential individualized encounters.
- A unified community school-based (vs. hospital or pharmacy based) campaign, fully engaging local families and their physicians in validating the safety and efficacy of a vaccine, and immunizing the general public.
Management came in the form of Basil O’Connor, attorney and close friend of the President. Their friendship predated FDR’s polio and included O’Connor serving as his legal adviser and for a brief period of time as his partner in the practice of law. He would serve loyally in that capacity for more than three decades as head of the National Foundation for Infantile Paralysis (NFIP).
O’Connor did not have an NIH or CDC to direct his efforts. He took charge himself, setting up an organizational structure with reach across the country to support services and fundraising. Ultimately, 3100 chapters would be established and $233 million distributed in patient services for children with polio by 1955.
On the research side, Jonas Salk was recruited to the University of Pittsburg in 1947. In 1948, he received a grant from the NFIP to identify the various types of polio. But Salk’s goals were much more expansive. He intended to develop the first successful vaccine for the disease and devoted the next seven years to that effort.
Fully funded by the NFIP at $7,500,000, and therefore requiring no need to be distracted by fund raising, Salk initiated a trial on 15,000 children in Allegheny County, Pennsylvania in 1953. The decision to stay close to home vastly simplified the logistics and avoided extra red tape. It didn’t hurt that he also tested himself, his wife and his children or that he achieved startling results on his first try out. Blood drawn from his subjects revealed antibody levels to polio that were 4 to 16 times the levels in non-treated children. These results were reported out in the Journal of the American Medical Association on March 25, 1953.
Following this announcement, which received worldwide attention, Salk took two additional steps that clearly demonstrated both his political and scientific prowess. First he went to Basil O’Connor at the NFIP and secured 100% funding for the largest scientific study that would ever be run in the US. In addition to securing that funding, he enlisted the vast marketing expertise and distribution system of the NFIP.
Secondly, rather than design the trials himself, at a time when scientific competitors were nipping at his heels, Salk enlisted his very popular and highly respected former mentor, Thomas Francis, to design and run the trials. Besides his scientific reputation, Francis had a distinguished record of public service having been the director of the Commission on Influenza for the Army Epidemiologic Board. By 1953, he was a renowned virologist and chair of the epidemiology department at the University of Michigan’s School of Public Health. Once Basil O’Connor with Salk chose Dr. Francis, they carefully created a firewall between themselves and the scientific trials.
Francis was fully aware of the deficiencies in the design. Did every parent clearly read the permission material? Clearly not. Was defining the trial’s purpose “to determine the effectiveness of a vaccine in preventing paralytic poliomyelitis” understating the trial’s experimental nature? What sufficed as a “valid parental signature”? Why were the terms “permission” and “human experiment” found nowhere on the consent form? Was Basil O’Connor’s letter on behalf of the NCIP that accompanied the parental materials and defined their child as having been “selected to take part in this great scientific test” overselling? And did he consciously underplay risk and deliberately transfer liability when he capitalized the words “THE VACCINE WILL BE GIVEN ONLY ON REQUEST OF THE PARENTS” in his letter?
My doctor father received a parcel post in his office in the Spring of 1954. It contained indistinguishable vials of the vaccine and placebo. He used the materials to inject the 2nd graders at our school, including my sister Pat. The event was memorialized in a front page photo in the local Hudson Dispatch of my father, needle in hand, and Pat wincing from the shot, but also proudly displaying her button and card declaring her a “Polio Pioneer”. That was Basil’s idea, as it was to give all the children who participated, including the controls who received no injections, buttons as well. In his view, no one should feel left out of this national public effort to beat the enemy – Polio.
The end results were startling and have never been replicated since. Beginning April 26, 1954, within a year’s time, 1.8 million children in 15,000 schools in 44 states were recruited for the experiment. 300,000 health professional volunteers, including my father and the majority of the physicians in the United States, participated without pay. 750,000 of the children – all 2nd graders form public and private schools – were part of a rigorous double blind study.
It was Dr. Francis who stood up on April 12, 1955 at 10:20 AM in Rackham Lecture Hall at the University of Michigan in Ann Arbor and declared in his characteristic direct style, “The vaccine works. It is safe, effective and potent.” The public trusted him at his word and complied with mass inoculations.
Tags: basil o'connor > covid > FDR > Pandemic > polio > public health > Salk > vaccines
Justice Is A Complicated Affair, Dr. Barrasso.
Posted on | January 28, 2021 | 4 Comments
Mike Magee
 Dr. John Barrasso, 1996, source/Spencer Books
Dr. John Barrasso, 1996, source/Spencer Books“We’re better than this” is the common refrain heard from many political leaders following the deadly assault on our democracy on January 6th. Are we really?
One year ago, my physician friend, Senator John Barrasso, famously said, “The time for political stunts is over. The Senate had a fair trial and clear acquittal. Republicans stayed true to the Constitution. Now the Senate gets back to work for the American people.” How did that work out for you, John?
This has been a week of empty appeals for blind appeasement and shifting of blame in the interest of “bringing our country together.” But as Senator Barrasso’s former colleagues in Medicine learned on their first day of Medical School, the only way to face bad news is to confront it, share it honestly with your patient and family, and together agree on the best curative course of action.
Justice is a complicated affair. A quick review of medical history is instructive – specifically Germany in 1945 and South Africa in 1995.
In sorting through the legacy of Hitler’s regime in Germany, the Allied forces established the International Military Tribunal. One of the series of trials, opened on November 19, 1945 in the Palace of Justice in Nuremberg, delved into egregious examples of medical criminality, including Nazi experimentation on human subjects. These trials are often cited as an example of “retributive justice.” Of 23 defendants, 7 were hanged, 7 acquitted, and the rest given sentences of from 10 years to life in prison.
These judgments were conducted under the direction of U.S. judges and prosecutors and fully compliant with U.S. standards of criminal procedure. Yet another 25 years would pass before any of the 10 agreed-upon medical ethics research standards were integrated into US trial law.
Legal scholars such as Michelle Miller at Cornell Law School attribute this lapse to the self-regarding biases of leaders within the Medical Industrial Complex. As Jay Katz, a physician and professor of law at Yale wrote in 1992 of the Nuremberg directives, “It was a good code for barbarians, but an unnecessary code for ordinary physician-scientists.”In other words, it was assumed that American medicine’s noble professionalism was adequate to ensure appropriate ethical standards.
Adding to the irony, at the very same moment that the leaders of the Medical Industrial Complex were rejecting President’s Truman’s 1946 call for a national health plan as “socialized medicine”, our military under the Marshall Plan was fast at work creating highly successful national health plans for our two main vanquished archenemies, Germany and Japan. We were willing to allocate precious taxpayer resources to assure this expression of “restorative justice.”
An analysis of the German and Japanese programs made some years later by the Rand Corporation summed up the Marshall Plan’s rationale: “Nation-building efforts cannot be successful unless adequate attention is paid to the health of the population. The health status of those living in the country has a direct impact on the nation’s construction and development, and history teaches us it can be a tool in capturing goodwill of the nation’s residents.”
A similar restorative approach was utilized in South Africa in 1995. Nelson Mandela’s Truth and Reconciliation Commission conducted over 1000 public hearings on their road to a free democracy, offering amnesty to those who publicly admitted past crimes of sectarian violence and asked for forgiveness. Less recognized, Mandela simultaneously instituted fundamental social service reform, including free primary level public health care for all in 1996 serviced in over 350 newly constructed health clinics by 1997.
The crimes of Donald Trump, his followers and enablers, are now fully exposed. Their failures include the mismanagement of the Covid-19 pandemic, certain to claim more than a half million Americans by April, 2021. As with Germany in 1945, and South Africa in 1995, these crimes involve racism, disinformation, and erosion of public trust. They are egregious, deep-seated, and likely not self-corrective.
To address them, and move our nation forward, we must openly and honestly embrace both retributive and restorative justice. Impeachment of Donald Trump, criminal investigations of his legislative and civilian co-conspirators, and movement toward universal health care in America are now important next steps if we truly wish to “bring our nation together.”
Tags: january 6 > restorative justice > retributive justice > Senator John Barrasso > trump > white supremacists
MLK (1967) to Biden (2021).
Posted on | January 21, 2021 | Comments Off on MLK (1967) to Biden (2021).

(a caution) “We are now faced with the fact, my friends, that tomorrow is today. We are confronted with the fierce urgency of now. In this unfolding conundrum of life and history, there is such a thing as being too late. Procrastination is still the thief of time. Life often leaves us standing bare, naked, and dejected with a lost opportunity. The tide in the affairs of men does not remain at flood — it ebbs.”
(a challenge) “This is the calling of the sons of God, and our brothers wait eagerly for our response. Shall we say the odds are too great? Shall we tell them the struggle is too hard? Will our message be that the forces of American life militate against their arrival as full men, and we send our deepest regrets? Or will there be another message — of longing, of hope, of solidarity with their yearnings, of commitment to their cause, whatever the cost?”
(and a choice) “The choice is ours, and though we might prefer it otherwise, we must choose in this crucial moment of human history…If we will but make the right choice, we will be able to speed up the day, all over America and all over the world, when justice will roll down like waters, and righteousness like a mighty stream.”
Latest State COVID Cases/Deaths/Vaccine Rates
Posted on | January 21, 2021 | Comments Off on Latest State COVID Cases/Deaths/Vaccine Rates
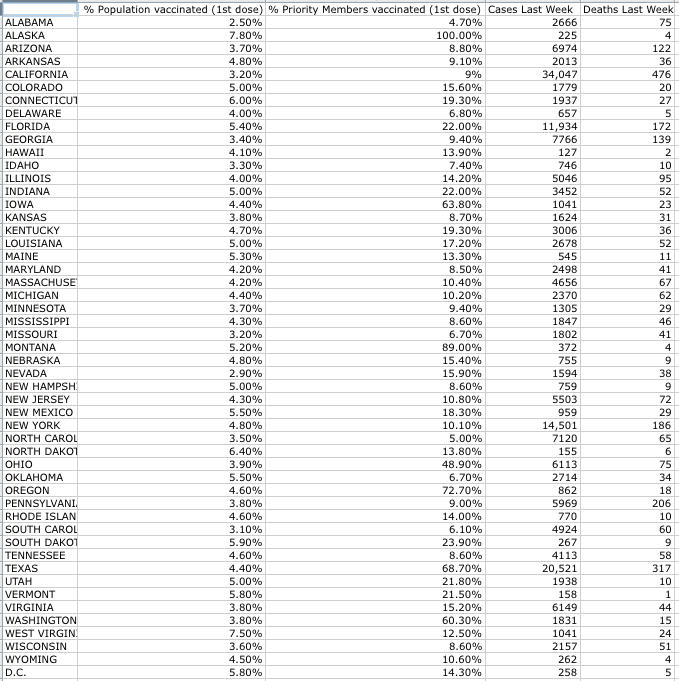
Data Source: Washington Post, 1/20/21
What MLK Said To President Biden on April 4, 1967.
Posted on | January 19, 2021 | 2 Comments

Mike Magee
Yesterday (in honor of Martin Luther King Day), and today (in prepartion for the Inauguration of our new President), I listened and re-listened to Dr. King’s famous Vietnam Speech at the Riverside Church in New York City on April 4, 1967.
I remembered this speech as a turning point in my sophomore year in a Jesuit College committed to social justice – the realization that justice travels down more than one path at a time – and that truth often hurts before it has a chance to help.
In the speech, King explains the origins of that evening in response to an earlier declaration by the leadership at Riverside Church. As he states, “I found myself in full accord when I read its opening lines: ‘A time comes when silence is betrayal.’…the calling to speak is often a vocation of agony, but we must speak.”
A little further on, he acknowledges his own followers discomfort with his outspoken position on Vietnam, with these words: “‘Why are you speaking about the war, Dr. King? Why are you joining the voices of dissent?’ ‘Peace and civil rights don’t mix,’ they say. ‘Aren’t you hurting the cause of your people?’ they ask. And when I hear them, though I often understand the source of their concern, I am nevertheless greatly saddened, for such questions mean that the inquirers have not really known me, my commitment, or my calling.”
By mid-speech, Dr. King reveals himself – to the audience that evening, but also to all of us now – having lived through January 6th and on the eve of President Biden’s inauguration. He says:
“In 1957, when a group of us formed the Southern Christian Leadership Conference, we chose as our motto: ‘To save the soul of America.’ We were convinced that we could not limit our vision to certain rights for black people, but instead affirmed the conviction that America would never be free or saved from itself until the descendants of its slaves were loosed completely from the shackles they still wear. In a way we were agreeing with Langston Hughes, that black bard of Harlem, who had written earlier:
O, yes, I say it plain,
America never was America to me,
And yet I swear this oath —
America will be!”
Near the end of his 1 hour oration, interrupted again and again by sustained applause, Dr. King asserts, “There is nothing to keep us from molding a recalcitrant status quo with bruised hands until we have fashioned it into a brotherhood… a genuine revolution of values means in the final analysis that our loyalties must become ecumenical rather than sectional…a fellowship that lifts neighborly concern beyond one’s tribe, race, class, and nation is in reality a call for an all-embracing and unconditional love for all mankind.”
And near the very end, he sees clear eyed to 2021, “speaking” to President Biden himself:
(a caution) “We are now faced with the fact, my friends, that tomorrow is today. We are confronted with the fierce urgency of now. In this unfolding conundrum of life and history, there is such a thing as being too late. Procrastination is still the thief of time. Life often leaves us standing bare, naked, and dejected with a lost opportunity. The tide in the affairs of men does not remain at flood — it ebbs.”
(a challenge) “This is the calling of the sons of God, and our brothers wait eagerly for our response. Shall we say the odds are too great? Shall we tell them the struggle is too hard? Will our message be that the forces of American life militate against their arrival as full men, and we send our deepest regrets? Or will there be another message — of longing, of hope, of solidarity with their yearnings, of commitment to their cause, whatever the cost?”
(and a choice) “The choice is ours, and though we might prefer it otherwise, we must choose in this crucial moment of human history…If we will but make the right choice, we will be able to speed up the day, all over America and all over the world, when justice will roll down like waters, and righteousness like a mighty stream.”
Latest State Covid Case/Deaths/Vaccine Rates
Posted on | January 13, 2021 | Comments Off on Latest State Covid Case/Deaths/Vaccine Rates
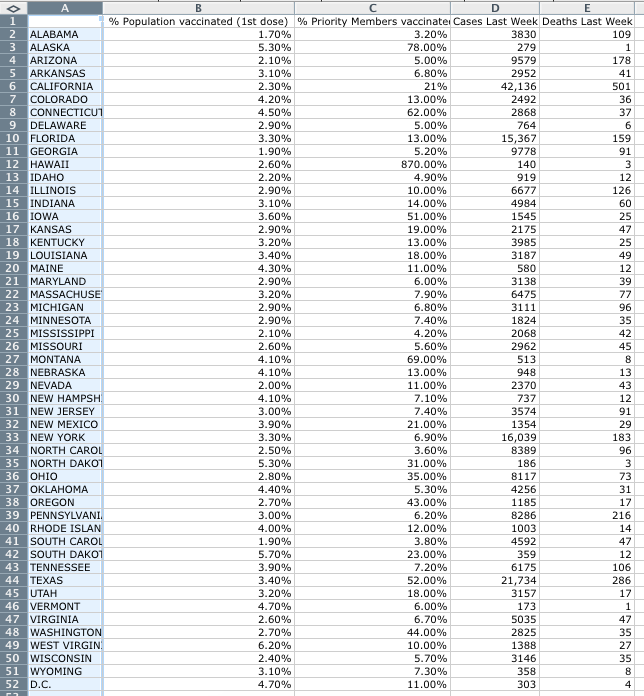
Data Source: Washington Post 11/13/21
Tags: covid > death rates > public health > state by state > vaccination rates
The Pathway Back.
Posted on | January 12, 2021 | Comments Off on The Pathway Back.

Marc Porter Magee, CEO, 50-CAN
Mike Magee
“We’re better than this” is the common refrain heard from many political leaders following the deadly assault on our democracy on January 6th. We here empty appeals for blind appeasement from the likes of Kevin McCarthy in the interest of “bringing our country together.” But for those who study history, pursuing this course takes our nation in exactly the wrong direction.
Rather, the model we must follow is the model of Germany in 1945, or South Africa in 1995. In both cases, strict legal and public accountability were married with fundamental expansion of universal social services to rebuild confidence and trust in their government’s ability to assure safety and security, and an equal playing field for all of their citizens.
Trump’s crimes have already helped carry our nation in the right direction in two ways:
1) They have revealed in word and image leaders and followers who actively engaged in insurrection. They must now be publicaly identified, charged, and feel the full weight of our law.
2) In counter-balance, these crimes have placed a spotlight on positive leaders and hopeful voices, ready to actively contribute to real healing and progress.
One such voice is my son, Marc Porter Magee, the CEO of the national educational advocacy non-profit 50-CAN. As their website says:
“To us, reimagining American K–12 education is more than a just cause, it’s the most important work we can do as a democracy. Equipped with nonpartisan research and proven tools, 50CAN citizen-advocates drive the creation of stronger, more equitable schools in every state and community in our network.”
Since the pandemic struck our schools, and entangled students and teachers alike, they have produced a weekly round-up of news and activities focused on solutions within the educational advocacy space, accompanied by Marc’s editorial. Here is his message this week:
“When we have written about our ‘new reality’ in this roundup the past 44 weeks, we have used that phrase to refer to a pandemic that has created an emergency situation for America’s school children.
“The insurrection that threatened the peaceful transfer of power in our nation’s capital last week is another kind of ‘new reality’–one that strikes at the heart of American democracy.
“The proximate causes are the actions of President Trump, who on the morning of January 6 directed the angry mob of supporters he had invited to Washington DC to march on to the Capitol, where a joint session of Congress was set to certify his loss. ‘You’ll never take back our country with weakness,’ he implored. ‘You have to show strength, and you have to be strong.’ A few hours later five people were dead, including 42-year-old police officer Brian Sicknick, who was bludgeoned to death by insurrectionists with a fire extinguisher. The hearings were cut short as our elected representatives fled for their lives and the Capitol building lay in shambles, the result of the first mass breach of its walls by enemies of our government since the War of 1812.
“As we wrote in the wake of the tragedy in Charlottesville in July 2017, ‘When you choose to march with Nazis you are rejecting our country’s founding belief that all people are created equal and dishonoring the basic convictions of the American political system. Because our common humanity binds us together, we also know that there aren’t two sides to this debate; only right and wrong.’
“By inciting violence to disrupt the transfer of power, Trump proved beyond any reasonable doubt he is unfit for his office. The correct response now is that he be impeached, removed and barred from ever holding elected office again.
“Whether the President is removed by Congress next week or simply leaves the nation’s capital when his term expires, we know that the threat to American democracy runs deeper than the flaws of one man. The collapse of trust in our country, the drumbeat of disinformation, the racism that twists institutions into instruments of oppression, ever-deepening political polarization and the increasing normalization of violence as a means of change have collectively brought us to the brink of disaster.
“There are no easy answers on our path out of the problems we face, yet we continue to believe that local advocacy–grounded in hope, committed to building bridges across divides, focused on delivering real change for communities in need–can make a difference. This, and the belief that Americans can and will overcome the forces of evil that attacked our democracy last week, are what inspire us to work at 50CAN.
“From civics to history to the critical thinking needed to separate fact from fiction, events like these are a reminder of how crucial it is for our children to receive an education that fully prepares them to uphold the great American experiment.
“That work continues in neighborhoods and statehouses across our network this week and the weeks to come in this new year.”
As Germany and South Africa learned, the pathway back to equality and humanity is a long one…but Trump, with criminal intent, has marked a beginning. Now we must, as a nation, see it to a successful end.
Tags: 50-CAN > Germany 1945 > healing > insurrection > marc porter mafgee > south africa 1995 > trump
"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
Homegrown Friends
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY

