Pope Francis, Skadden, Scalia and “Due Process.”
Posted on | April 22, 2025 | No Comments
Mike Magee
“If our church is not marked by caring for the poor, the oppressed, the hungry, we are guilty of heresy.”
― St. Ignatius of Loyola, Founder of the Jesuit Order
The Pope’s passing interrupted an epic battle between Trump and the rest of the civilized world over whether America remains a society “under the law.” Critical to the rule of law is the principle of “Due Process,” as described in not one, but two Amendments to our Constitution.
The Fifth Amendment states that no inhabitant shall be “deprived of life, liberty or property without due process of law.”
The Fourteenth Amendment, ratified after the Civil War and Emancipation, uses the same eleven words, called the “Due Process Clause,” to describe a legal obligation of all states.
In arrogantly ignoring any pretense of “Due Process” last week by deporting accused (but not proven) alleged gang member Kilmar Abrego Garcia to an El Salvador top security prison along with 220 others, and ignoring a court order to return the planes while still in flight, Trump basically thumbed his nose at America’s legal system. This was a bridge too far, even for some of his political supporters in Congress.
With that case still in litigation, the Administration tried to repeat the publicity stunt with another group of accused aliens this past weekend and was slapped down by the Supreme Court in an unanimous decision.
What Trump is learning the hard way is that without “Due Process” the law profession might as well hang up its shingle. Trump thought he had Chief Justice Roberts in his pocket when he purposefully allowed himself to be caught on a hot mic as he passed the Chief Justice on his way to deliver the 2025 State of the Union Address. His words for the camera, “Thank you again. Thank you again. Won’t forget it.” were intended to signal to the world, He owes me big time, and I own him.
A common “Due Process” thread connecting these two current events (the Pope’s death and the illegal deportation of Kilmar Albrego Garcia) includes another Supreme Court Justice – Antonio Scalia. Catholic and trained by Jesuits, he shared a common lineage with Pope Francis, the first Jesuit ever to lead the Catholic Church. Other Justices also share this Jesuit educational parentage including Clarence Thomas, Brett Kavanaugh, and Neil Gorsuch.
But Francis and Antonin have a second historical connection. Pope Francis, the day before the 2025 State of the Union address, publicly labeled the immigration policies of the incoming President and Vice President, “a disgrace.” More recently, the Vatican spoke out in opposition to last weeks El Salvador imprisonments. Part of criticism tracks back to the lack of “Due Process.”
Glaringly obvious today, this was just one arm of an aggressive Project 2025 campaign against America’s Legal Profession. By late March, multiple DC based law firms pledged allegiance to the Trump Administration to avoid being barred from entering Federal buildings to represent their clients. Some members of the targeted firms resisted. For example, Skadden associate, Rachel Cohen, resigned from her firm in protest, stating, “It does just all come around to, is this industry going to be silent when the president operates outside the balance of the law, or is it not?”
Former Skadden alumni spoke out in mass along with Rachel this week. Eighty plus former associates of the firm signed on to a letter of public protest that stated in part, “As alumni of Skadden, we write to express our profound disappointment and deep outrage regarding the firm’s recent agreement with President Donald Trump. At a time when rule of law, freedom of speech, and the adversarial system collectively face existential threat, Skadden’s agreement with President Trump emboldened him to further undermine our democracy.”
As it turns out, one current Skadden Associate’s voice, from 9 years ago when she was still a student at Harvard Law, has brought legendary conservative justice, Antonin Scalia, into the mix. Back then Lucy Dicks-Mireaux described herself as “a liberal, minority woman” who believed that “many of Justice Scalia’s opinions set equality back several decades—further back than his three decades on the Court would suggest.”
But she wrote in the May 4, 2016 issue of the “Harvard Civil Rights-Civil Liberties Law Review,” that she had a partial change of heart “when I read Justice Scalia’s dissent in Hamdi v. Rumsfeld (and found) that I agree with him.”
As Dicks-Mireaux went on to explain at the time: “In Hamdi, the U.S. military detained Hamdi, a U.S. citizen, in the United States as an ‘enemy combatant‘ without a trial. The military believed Hamdi to be working with the Taliban, but did not bring a criminal suit against him. Hamdi’s father filed a writ of habeas corpus, a petition asking Hamdi to be delivered to the court or released absent a trial. The majority opinion curtailed Hamdi’s due process right by allowing him to be detained with a meager showing by the government of evidence that they had a reason to hold Hamdi. The tribunal before which Hamdi would be afforded a chance to rebut these allegations would not be a court of law, but a neutral decision maker. Hearsay evidence would be allowed. Hamdi would be presumed guilty until proven innocent.”
In a prescient remark that followed, we see how relevant her analysis a decade ago is to the current battle to return Kilmar Albrego Garcia. She states, “I was very disturbed by the extent to which the Court would curtail an essential constitutional right—due process—in the face of vague national security concerns.”
To her surprise, so was Justice Scalia. As she explained, “The voice of reason came from an unexpected source: Justice Scalia. Arguing that the government could not hold citizens unless the government prosecuted them, Justice Scalia would have granted habeas corpus (fundamental protection against unlawful detention). Justice Scalia would have required that the government either promptly bring charges against Hamdi in a court of law, or Congress would have to suspend habeas corpus. I could not believe that Justice Scalia was advocating for the little guy, but here he was, in black and white, writing that Hamdi deserved better than what the court had offered. Hamdi deserved better because the law required it.”
Attorney Dicks-Mireaux joined Skadden after graduating from Harvard Law School in 2018. She is an Associate in their Litigation Department, and in 2023, she received “High Honors” by the DC Courts for her “Pro Bono” work. Will her skills be put to Trump’s use in the future?
As many top lawyers in the United States, and religious leaders within the Catholic Church and beyond well understand, human rights are not only God-given, but also intended to be vigorously defended under the “Due Process Claus” of our Constitution. If we fail in this regard, we can hardly claim to be just citizens of these United States. As St. Ignatius Loyola said, and his disciple Pope Francis embodied to the very end, “If our church is not marked by caring for the poor, the oppressed, the hungry, we are guilty of heresy.”
Tags: 14th amendment > 5th amendment > Catholic Church > due process claus > hamdi v. rumsfeld > Lucy Dicks-Mireaux > Pope Francis > skadden > trump > Vance
The Birth of The Germ Theory
Posted on | April 21, 2025 | No Comments
Mike Magee
When Yellow Fever broke out shortly after the arrival of a trading ship from Saint-Dominque in Philadelphia among colonists with no immunity in 1793, the main response was panic, fear, and mass evacuation from the city. Five thousand citizens, roughly 10% of the population, including Alexander Hamilton and his wife, fled. Experts were at a loss to explain the cause, and were even more confused how to treat the disease.
Benjamin Rush was the primary leader of Medicine in the young nation where physicians were scarce and nearly all relied on Europe for their advanced education. In confronting the epidemic, Rush believed the problem involved a disturbance of the four humors – blood, phlegm, black bile and yellow bile. His solution was the rather liberal and barbaric use of cathartics and blood letting. For the most severe cases, Rush warehoused dying victims in the first “fever hospital” in the new nation.
But a century later, as historian Frank Snowden wrote, “Humoralism was in retreat as doctors absorbed ideas about the circulatory and nervous systems, and as the chemical revolution and the periodic table undermined Aristotelian notions of the four elements composing the cosmos…More change occurred in the decades since the French Revolution than in all the centuries between the birth of Socrates and the seizure of the Bastille combined.”
During the 20th century, but especially in the second half of the 1800’s, scientific progress was self-propagating. Much of the credit for this enlightened progress goes to the rapid evolution of “the germ theory.” No single genius was responsible. Rather, knowledge built step wise and involved a collective (if not fully cooperative) effort by multiple scientists.
One of the early insights was that late stage disease in morbid hospitalized patients literally “on their last leg” was the tail end of a process. French physiologist, Claude Bernard in his “An Introduction to the Study of Experimental Medicine,” made the point that the challenge was to uncover the “beginnings” of these “final stages.” Rather than observe dying bedridden patients, he promoted “experimentalism medicine” in outside laboratories. In doing so, Bernard was likely not fully aware that he was tipping the national scale of medical discovery toward Germany where scientific and research laboratories enjoyed popular support.
It’s important to note that leaders at the time were not intellectual elites, but rather more often skilled artisans of the natural world. A prime example was Antonie van Leeuwenhoek who opened his first store as a cloth merchant at the age of 22 in 1654. Prior to this, he had served as an apprentice to a lens grinder and metalworker. It was in pursuit of a better view of the threads of cloth he was purchasing and selling that he devised one of the first single lens microscopes which had a magnification of 275X.
His curiosity spilled over to the natural world as well. And so it was that he noted in a liquid specimen single cell organisms he labeled “animalcules” in a poorly received communication to the Royal Society of London at the age of 44 in 1676. After a year of hedging, the Royal Society finally acknowledged such creatures existed.
But another seventy years would pass before a connection was made between microscopic “animalcules” and disease. The insight came thanks to the dogged experimentation of an Hungarian gynecologist who put 2 and 2 together in 1847. Maternal mortality from “puerperal fever” was commonplace at Vienna General Hospital at the time. But Ignaz Philipp Semmelweis, the physician director of the service, noticed that mortality rates between his two service – one run by physicians and the other midwives – was strikingly different. (20% vs. 2%). Delivery practices were roughly the same. But one difference stuck out. The physicians also were in charge of mandatory autopsies, and often shuttled between the delivery suite and morgue without a change in clothing or any cleansing whatsoever. Also one of Semmelweis’s trainees who cut himself during an autopsy also died of an identical disease. So he decided to require that members of both team would wash their hands in a chlorine solution before entering the maternity area. Mortality rapidly dropped to 1.3%.
Others were making the connection as well. For example, few stories are as well known as the case of John Snow, the London public health pioneer, who in 1854, traced the death of 500 victims during a cholera epidemic to a contaminated Broad Street water pump. Removing the pump handle was curative. As important as the investigative findings were his publication the following year titled “On The Mode of Communication of Cholera” because scientific progress relies heavily on transfer of knowledge and sequential collaboration. That same year, an Italian physician, Fillippo Pacini, first visualized the organism. But 3 more decades would pass before the German physician, Robert Koch, would isolate the bacterium in pure culture.
Koch was one of “The Famous Trio,” credited by historian Frank Snowden with creating “a wholesale revolution in medical philosophy.” In addition to Koch, these included French scientist Louis Pasteur and Scottish surgeon, Joseph Lister.
I. Louis Pasteur (1822-1895) was a French chemist (not a biologist or physician) who famously stated that “Where observation is concerned, chance favors only the prepared mind.” In the 1850s, while investigating spoilage of wine and milk, he developed the theory that putrefaction and fermentation were not “spontaneous”, but the result of bacterial processes, and that these degrading actions could be altered by heat. Heat destroyed the bacteria, and prevented spoilage (ie. pasteurization). This insight launched the field of “microbiology”.
Pasteur also helped define the principles of “nonrecurrence” (later called “acquired immunity”), and “attenuation”, a technique to render microbe causing disease specimens harmless when introduced as vaccines.
II. Robert Koch (1843-1910) was a German physician 20 years younger than Pasteur. He investigated Anthrax in the mid-1870’s at the University of Gottingen. Luckily the bacterium was very large and visible with the microscopes of the day. He was able to reproduce the disease in virgin animals by injecting blood from infected sheep. But, in addition, he detected and described spores formed by the bacterium, which were left in fields where infected animals grazed. The spores, he declared were why virgin animals grazing in these fields, became infected.
Teaming up with the Carl Zeiss optical company, Koch focused on technology, improving magnification lens, developing specialized specimen stains, and developing fixed culture media to grow microbes outside of animals. Armed with new tools and stains, he discovered the Mycobacteria tuberculosis and proved its presence in infected tissues, and described his findings in “The Etiology of Tuberculosis” in 1882.
“Koch’s Postulates” became the 4 accepted steps constituting scientific proof of a theory.
1) The microorganism must be found in infected tissue.
2) The organism must be grown in fixed culture.
3) The grown organism must instigate infection in a healthy laboratory animal.
4) The infective organism must be re-isolated from the lab animal, and proven identical to the original microbes.
III. Joseph Lister (1827-1912), the third of our trio, was a professor of surgery at Edinburgh. At the time, major complications of surgery were pain, blood loss and deadly post-operative infections. In the 1840s, ether and nitrous oxide were introduced, controlling intra-operative pain. As for infection, Lister suggested scrubbing hands before surgery, sterilizing tools, and spraying carbolic acid into the air and on the patient’s wound. Koch took an alternate approach, advocating sterile operating theories and surgeons in gowns, gloves, and masks. The opposing techniques merged and became common surgical practice in the 1890s.
For New York City, Chadwick’s sanitary movement and the “famous trio’s” germ theory couldn’t arrive soon enough. The Civil War had been a wake-up call. Of the 620,000 military deaths, 2/3 were from disease. At the top of the list was dysentery and diarrheal disease, followed by malaria, cholera, typhus, smallpox, typhoid and others. Filth, disease, and disorder ruled the day. But opportunity lay in the wings. As historians described the challenge of those days: “New York City experienced a pivotal moment in its development following the historic 1898 consolidation, which united Manhattan, Brooklyn, Queens, The Bronx, and Staten Island into one comprehensive entity. By the year 1900, the city’s population had surged to 3,437,202 according to the U.S. Census.” Keeping those millions healthy would be a public health challenge of the first order.
The Birth of The Sanitation Movement from “Dirty Old London” to NYC.
Posted on | April 10, 2025 | Comments Off on The Birth of The Sanitation Movement from “Dirty Old London” to NYC.
Mike Magee

I. Florence Nightengale and Sidney Herbert
Order had always been part of Florence Nightingale’s life. Her father was William Edward Shore, a Country Squire, who at age 21 inherited his rich uncle’s huge fortune as well as his name. On his death, the younger (now) Nightingale, seamlessly managed the profits of the family’s lead smelting business, as well as, not one, but two named estates – the 1300 acre Lea Hurst in Derbyshire, and the equally impressive Embry Park in Hampshire.
He and his wife had two daughters, each named after the Italian cities where they were born while vacationing. Parthenope carried the Greek name for Naples, and Florence arrived on May 12, 1820, one year later 300 miles north in the “Birthplace of the Renaissance.” The family was well connected with members of Parliament, none closer than Baron Sidney Herbert. It was he who the family turned to for reassurance and guidance when Florence declared at age 16 that her life’s work would be nursing the sick and ill in the service of the Lord.
This was quite a surprise to her father who had taken special care to see that she was classically trained in Greek, Latin, French, German, Philosophy and Religion. But in Florence’s words, she “craved for some regular occupation, for something worth doing instead of frittering away time on useless trifles.” To do so, she was willing to decline suitors and her mother and older sister’s life of comfort and philanthropy.
Sidney Herbert was willing to support the strong willed woman, 10 years his younger, carrying her along on fact-finding trips to Egypt and beyond. None of it shook her commitment. Her intent was clear when she noted in her diary, “On February 7, 1837, God spoke to me and called me to his service.” The calling was specific – nursing the ill in institutional settings. As luck would have it, her goal aligned well with the voluntary efforts of Sidney’s wife, the Lady Elizabeth Mary Herbert, a prodigious fund raiser.
Queen Victoria assumed the throne of England following her Uncle’s death just 4 months after Florence’s religious awakening. The two were born exactly 1 year and 12 days apart. Both the young Queen and her husband, Albert, were military enthusiasts, and saw themselves as active participants in the nation’s armed conflicts. In September, 1854, they had a front row seat in a simmering conflict between the Ottoman Empire and Russia. Britain and France had thought they had brokered a deal between the two primary combatants when the truce fell apart.
Russian Emperor, Nicholas I, then ordered the invasion of what is now current day Romania in July of 1853. By January, 1854, the British and French fleets had entered the Black Sea, and the war was on. Britain’s Prime Minister, Lord Palmerston, suggested the effort was preventive. As he said in words that ring true today, “The main and real object of the war is to curb the aggressive ambition of Russia.”
Military historians would later document: “The Crimean War is largely forgotten now, but its impact was momentous. It killed 900,000 combatants; introduced artillery and modern war correspondents to conflict zones; strengthened the British Empire; weakened Russia; and cast Crimea as a pawn among the great powers.”
At the time, Queen Victoria leaned heavily on her new Secretary of War, Sidney Herbert, and Florence Nightingale saw a once in a lifetime opportunity for clinical experience and seized it. With Herbert’s endorsement, she and the 38 nurses in her charge arrived at Barrack Hospital at Scutari, outside modern day Istanbul, ill prepared for the disaster that awaited them. Cholera, dysentery and frostbite – rather than battle wounds – were rampant in the cold, damp, and filthy halls.
During that first winter, 42% of her patients perished, leaving over 4000 dead, the vast majority absent any battle wounds. Florence later described her work setting as “slaughter houses.” Their enemy wasn’t bullets or bayonets, but disease -typhus, cholera and typhoid fever. Over 16,000 British soldiers died, 13,000 from disease.
Nightingale’s initial assessment was that warmer clothing and food would stem the tide. Going over the heads of medical leadership, she did what she could, and leaked details of what she was observing to Herbert and journalists who, for the first time, were stationed within the war zone. In the process, she became a celebrity in her own right, and as Spring of 1855 approached, a first ever Sanitary Commission was sent to the war zone and Victoria and Albert themselves, with two of their children, visited the area.
Famed artist Jerry Barrett made hasty sketches of what would become The Mission of Mercy: Florence Nightingale, which hangs to this day in the National Gallery in London. During this same period, the first lines of Henry Wadsworth Longfellow’s poem, Santa Filomena, would take shape, including “Lo! In that house of misery, A lady with a lamp I see, Pass through the glimmering of gloom, And flit from room to room.” And the legend of Nightingale, the actual “Lady of the Lamp”, appeared on the front page of the Illustrated London News complete with etched images.
It read: “She is a ministering angel without any exaggeration in these hospitals, and as her slender form glides gently along each corridor, every poor fellow’s face softens with gratitude at the sight of her.”
What became clear to Florence and others was that infection and lack of sanitation were the culprits, and corrective actions on the facilities themselves, along with sanitary practices that Nightingale led, caused the subsequent mortality rates to drop to 2%. By the time the war drew to a halt in February, 1856, 900,000 men had died. Florence Nightingale remained for four more months, arriving home without fanfare on July 15, 1856. Thanks to the first ever war correspondents, she was now the 2nd most famous woman in Britain, after Queen Victoria.
While she was away, the Herberts raised money from rich friends. The Nightingale Fund now had 44,000 pounds in reserve. These would help fund a hospital training school and her famous book, “Notes on Nursing” in future years. Though her re-entry was quiet and reserved, she had plenty to say, and committed most of it to writing. While in Crimea, she had written to Britains top statistician, Dr. William Farr. He had replied, “Dear Miss Nightingale. I have read with much profit your admirable observations. It is like light shining in a dark place. You must when you have completed your task – give some preliminary explanation – for the sake of the ignorant reader.” Shortly after her return, they met. Working closely with William Farr, she documented in dramatic form, the deadly toll in Crimea and tied it to disease and lack of sanitation in “Notes Affecting the Health, Efficiency, and Hospital Administration of the British Army”, which she self-published and aggressively distributed.
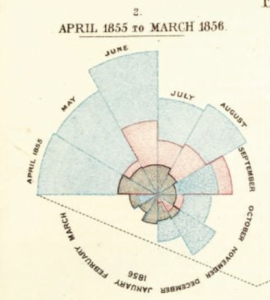
Illustrated with spin wheel designs divided into 12 sectors, each one representing a month, she graphically tied improved sanitation to plummeting death rates. Understanding their long-term value, she carefully approved the paper, ink, and process that have allowed these images to remain vibrant a century and a half later. As she said later with some cynicism, they were “designed ‘to affect thro’ the Eyes what we may fail to convey to the brains of the public through their word-proof ears.” In 1858, she became the first woman to be made a fellow of the Royal Statistical Society.
In that first year of her return, she was described as “a one woman pressure group and think tank…using statistics to understand how the world worked was to understand the mind of God.”In 1860, she published her “Notes for Nursing,” selling 15,000 copies in first two months. It purposefully championed sanitation (“the proper use of fresh air, light, warmth, cleanliness, quiet, and the proper selection and administration of diet”) and promoted cleanliness as a path to godliness. It targeted “everywoman” while launching professional nursing.
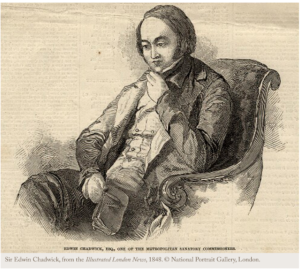
II. Edwin Chadwick
Florence Nightengale was not the originator of the Sanitary Movement in “Dirty Old London.” That honor goes to one Edwin Chadwick, a barrister who, in 1848, published his “Report on the Sanitary Condition of the Laboring Population of Great Britain.” As historians and commentators have noted, there was a good case to be made for cleanliness. Here are a few of those remarks:
“The social conditions that Chadwick laid bare mapped perfectly onto the geography of epidemic disease…filth caused poverty, and not the reverse.”
“Filthy living conditions and ill health demoralized workers, leading them to seek solace and escape at the alehouse. There they spent their wages, neglected their families, abandoned church, and descended into lives of recklessness, improvidence, and vice.”
“The results were poverty and social tensions…Cleanliness, therefore, exercised a civilizing, even Christianizing, function.”
Chadwick was born on January 24, 1800. His mother died when he was an infant, and his father was a liberal politician and educator. His grandfather was a close confidant of Methodist theologian, John Wesley. Early in his life, young Chadwick pursued a career of his own in law and social reform. A skilled writer, one of his early essays that appeared in the Westminister Review was titled “Applied Science and its place in Democracy.” By the time he was 32, he focused all of expertise on social engineering – especially public health with an emphasis on sanitation
But the Sanitary Movement required population-wide participation, structural change, new technology, and effective story telling. By then, Sir William Harvey’s description of the human circulatory system in 1628, complete with pump, outlet channels, and return venous channels, was well understood by most. Seizing on the analogy, Chadwick, along with city engineers of the day, imagined an underground highway of pipes, to and from every building and home, whose branches, connected to new sanitary devices.
One of those engineers was George Jennings, the owner of South Western Pottery in Dorset, the maker of water closets and sanitary pipes. He was something of a legend in his own time, and recipient of the 1947 Medal of the Society of Arts presented by none other than Prince Albert himself.
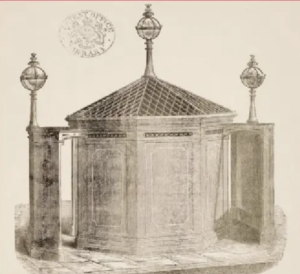
When Jennings patented the first toilet, as a replacement for soil pots, hand transported each mornings and emptied in an outhouse if you were lucky, or in the streets if not, its’ future was anything but assured. But, by good luck, the Great Exhibition (the premier display of futuristic visionaries) was scheduled for London in 1851. The Crystal Palace exhibition was the show stopper, attracting a wide range of imagineers. Jennings “Monkey Closet” was the hit of the show. His patent application followed the next year and read: “Patent dated 23 August 1852. JOSIAH GEORGE JENNINGS, of Great Charlotte – street, Blackfriars-road, brass founder. For improvements in water-closets, in traps and valves, and in pumps.”
Modernity had arrived. And none was more enthusiastic than Thomas Crapper, a then 15-year old dreamer. Within three decades he had nine toilet patents, including one for the U-bend, an improvement on the S-bend, and an 1880 Royal commission granted to Thomas Crapper & Co. to install thirty toilets(enclosed and outfitted with cedar wood seats in the newly purchased Norfolk county seat’s Sandringham House. His reputation lives on thanks to this diminutive term, used with the greatest guttural emphasis by the Scots – CRAP. The company is also still in existence, now selling luxury models of the original design.
Sanitary engineering combined with Nightingale’s emphasis on fastidious housekeeping, and cleanliness in hospitals, enforced by nurses with religious zeal, would change the world. And they did. But those same changes would take decades to reach crowded immigrant entry points in locations like New York City.

III. The Horse and Swill Milk
One historian described it this way, “As New York City ascended from a small seaport to an international city in the 1899’s, it underwent severe growing pains. Filth, disease, and disorder ravaged the city to a degree that would horrify even the most jaded modern urban developer.”
One of the prime offenders was the noble work horse. By 1900, on the eve of wholesale arrival of motor cars, there were roughly 200,000 horses in New York City, carrying and transporting humans, and products of every size and shape, day and night along the warn down cobble stone narrow roads and alley ways.
It was a hard life for the horse, who’s lifespan on average was only 2 1/2 years. They were literally “worked to death.” In the 1800’s, 15,000 dead horses were carted away in a single year. Often, they were left to rot in the street because they were too heavy to transport. If they weren’t dying, the horses were producing manure – a startling 5 million pounds dumped on city streets each day.
As for human waste, sewer construction didn’t begin in New York until 1849, this in response to a major cholera outbreak. Clean water had arrived seven years earlier with the arrival Croton Aqueduct carrying water south from Westchester County. This was augmented with rooftop water tanks beginning in 1880. By 1902, most of the city had sewage service including the majority of the tenement houses. The Tenement Act of 1901 had required that each unit have at least one “water closet.”
As for the horses, the arrival of automobiles almost eliminated the “horse problem” overnight. Not so for cows, or more specifically the disease laden “swill milk” cows. Suppliers north of the city struggled to keep up with demand in the late 1800’s. To lower production costs, they fed their cows the cast off “swill” of local alcohol distilleries. This led to infections and a range of diseases in the bargain basement beverage sold primarily to at-risk parents and consumed by children.
Swill milk was the chief culprit in soaring infant mortality in New York City between 1880 and 2000. Annually there were some 150,000 cases of diphtheria, resulting in 15,000 deaths a year. A Swiss scientist, Edwin Klebs, identified the causative bacteria, Corynebacterium diphtheriae, in 1883. A decade later, a German scientist, Emil von Behring, dubbed the “Saviour of Children” developed an anti-toxin to diphtheria and was awarded the Nobel Prize in 1901for the achievement.
The casualties were primarily infants whose mortality rate in NYC at the time was 240 deaths per 1000 live births. Many of these would be traced back to milk infected with TB, typhoid, Strep induced Scarlet Fever and Diphtheria. The casualties were primarily infants whose mortality rate in NYC at the time was 240 deaths per 1000 live births.
The process of heating liquid to purify it, or pasteurization, was discovered by Louis Pasteur in 1856, not with milk but with wine. Its’ use on a broad scale to purify milk first gained serious traction in 1878 after Harper’s Weekly published an expose’ on “Swill Milk.” But major producers and distributors resisted regulation until 1913 when a massive typhoid epidemic from infected milk killed thousands of New York infants. But diphtheria remained the most feared killer of infants.
As Paul DeKruif wrote in his 1926 book, The Microbe Hunters, “The wards of the hospitals for sick children were melancholy with a forlorn wailing; there were gurgling coughs foretelling suffocation; on the sad rows of narrow beds were white pillows framing small faces blue with the strangling grip of an unknown hand.”
One such victim was the only child of two physicians, Abraham and Mary Putnam Jacobi whose 7-year old son, Ernst, was claimed by the disease in 1883. Working with philathroper, Nathan Straus, the Jacobi’s established pasteurized milk stations in the city which coincided with a 70% decline in infant mortality from diphtheria, tuberculosis and a range of other infectious diseases.
By 1902, the horses hero status was reclaimed as it became the source of diphtheria and tetanus anti-toxins. The bacteria were injected into the horses, and after a number of passes, serum collected from the horse was laden with protective anti-toxins, relatively safe for human use. In 1901 alone, New York City purchased and delivered 25,000 does of ant-toxin funded by the Red Cross and the Metropolitan Life Insurance Company.
Tags: crimean war > edwin chadwick > florence nightingale > george jennings > jacobi > monkey closet > nicholasI > nightingale fund > queen victoria > santa filomena > sidney herbert > straus > the microbe hunters > thomas crapper > william edward shore > william farr
“Think Microscopically” – The Birth of Cell Theory.
Posted on | April 8, 2025 | 2 Comments
Mike Magee
If there was an All-Star team for 20th Century Medicine, two members of the roster would likely be William Welch and William Osler, two of the “Big Four” founders of the Johns Hopkins School of Medicine. (The other two were surgeon William Stewart Halsted and obstetrician Howard Atwood Kelly.) Welch served as the first Dean of the school and Osler, born and bred in Canada, arrived at Johns Hopkins at the age of 40, and birthed the first residency training program at the school.
Prior to their arrival in Baltimore, the two shared a common medical origin story. They both were trained in pathology and cell theory by the famed German physician, Rudolph Virchow. He encouraged them both to embrace “attention to detail” by “thinking microscopically.”

Virchow is remembered for a famous phrase – “omnis cellula e cellula” (every cell stems from another cell). That may not sound too radical today. But back in 1855, it was revolutionary. Cells, as an entity, had been around for awhile. Two centuries earlier, in 1665, English scientist Robert Hooke, while observing a dead specimen of cork under a microscope, noted that the repetitive compartments reminded him of monk’s rows of rooms or cellula in a monastery. When he published that impression in Micrographia that year, the label “cell” was born.
He was not the first to use a microscope. That honor remains contested. But it is known that the first use of a compound microscope (an instrument which married an eye piece with an objective lens positioned near the specimen) dates to at least 1619. A half century later, in 1674, Anton van Leeuwenhoek, the Dutch scientist, first described a living algae and bacteria cells.
Over the next two centuries, cells were seen here, there, and everywhere, without many conclusions drawn. But in 1838, two German scientists – zoologist Theodor Schwann and botanist Matthias Schleiden – noted the similarities of plant and animal cells in a wide range of observed tissues. A year later, Schwann published a book claiming that: 1) The cell is the fundamental unit of structure and function in living things, and 2) All organisms are made up of one or more cells. In pushing his third insight, that new cells emerged through a process of “spontaneous generation” like crystal formation from an original cell, he found himself “a bit over his skies.” But Virchow happily corrected him 17 years later in 1855 with his “omnis cellula e cellula.”
With this insight, Virchow launched the field of cellular pathology. How exactly cells manage to divide and create identical copies of themselves remained to be determined. Bit he did figure out, before nearly all other scientists, that diseases must involve distortions or changes in cells. From this he deduced that diagnosis and ultimately treatment could now be guided not simply by symptoms or external findings, but by cellular pathologic changes as well. And this was more than theory. In fact, Virchow is credited with first describing the microscopic findings of leukemia way back in 1847.
The first description of a cell nucleus was made by a Scottish botanist, Robert Brown in 1833. Over the next half-century, cell scientists busily described various cell organelles without a clear understanding of what they did. What was clear with light microscopy was that cells were bounded by a cellular membrane.
Most of the attention in the second half of the 19th century was on the nucleus and its division and cell replication. In 1874, German biologist, Walther Flemming first described mitosis in detail. But it wasn’t until 1924 that German biologist Robert Feulgen, “following experiments using basic stains such as haematoxylin, defined chromatin as ‘the substance in the cell nucleus which takes up color during nuclear staining’”. To this day, the Feulgen reaction “still exerts an important influence in current histochemical studies.”
Watson & Crick’s description of the DNA double helix was still far in the distance. But in the mean time, other cell organelles were visualized and named like the Golgi apparatus named in 1898 after Italian biologist Camillo Golgi who also used heavy metal stains (silver nitrate or osmium tetroxide) to aid visualization. Mitochondria, like the Golgi apparatus, stretched the limits of light microscopic visualization. But even without visualization, scientists by the 1930’s were beginning to deduce the functions of organelles they could barely see, and a few (like lysosomes) that they had never seen but knew had to be there.
The electron microscope popularization (if not its discovery) is generally credited to two German PhD students, Max Knoll and Ernst Ruska, who used two magnetic lenses to generate a beam of electrons and achieve much higher magnifications in 1931. For their efforts they received the 1986 Nobel Prize in Physics. Breakthroughs began to roll out almost immediately. High resolution pictures of mitochondria appeared in 1952, followed by the Golgi apparatus in 1954. The inner workings of the cells displayed movement of vesicles across the membrane and from nucleus to cytoplasm, with structures constantly being constructed and deconstructed. And visualization only got better in 1965 when the first scanning electron microscope went commercial.
Cells vary enormously in size. The smallest free-living cellular organism is the mycoplasma bacterium. It lacks a cell wall (important since many antibiotics work against bacteria by disrupting their cell walls) and is 400,000 times smaller than a human cell. A full-grown human organism includes some 30 trillion cells. Each cell is remarkably complex, holding about 10,000 different proteins, but possessing enough directions within its DNA manual to produce up to 100,000 protein varieties. The extra 90,000 are only employed in “specialized cells.” Order is maintained inside the cell by membrane sub-compartmentalization. Specialization is reflected in the choice of macromolecules that are allied by function.
Keeping individual 30 trillion cell human collections alive was part of my learning curve as a surgical resident at the University of North Carolinas from 1973 to 1978. Our Chief of the Trauma Department was a Vietnam veteran, Dr. Herb Proctor. As the Level 1 trauma facility, the sound of helicopters overhead was a constant. And victims arriving often needed fluids fast. One of the intravenous fluids of choice was “Ringers lactate,” a substance that included sodium chloride, potassium chloride, calcium chloride and sodium bicarbonate.
The life saving formula was created by a British physician named Sydney Ringer in 1882. He came up with the formula for Ringer’s Lactate while experimenting on how to keep a frog heart (removed from the frog) beating while suspended in solution. Three years later, a budding German embryologist, Wilhelm Roux, who was fixated on “showing Darwinian processes on a cellular level,” was able to keep cells he had extracted from a chicken embryo alive for 13 days. With that, the discipline called cell culture or tissue culture was off and running.
In modern usage, the term refers to growing cells from a multicellular organism outside the body, or in vitro. Bathed in special culture medium, naturally or scientifically mutated cells, can grow and continue to divide indefinitely, creating an immortalized cell line. In the early years, these cell lines were often contaminated by other types of cells, or more commonly by infectious organisms. The discovery of antibiotics by Alexander Fleming in 1928 greatly improved the reliability of the use of these cell lines for scientific experimentation.
With the introduction of living cell cultures, and the use of the electron microscope, the inner workings of the cell were revealed. Simultaneously, the field of biochemistry matured, alongside the miracle of genetics. Side by side, in direct view, fertilization, embryonic development, multi-potential stem cells with timed specialization, organ development, and ultimately Watson and Crick’s description (building on the work of Rosalind Franklin and Maurice Wilkins) of the DNA double helix in 1953 opened the doors a half century later to the sequencing of the human cell genome in 2003 after a 13 year race to the finish line by competitors, then collaborators, NIH lead Francis Collins and the Celera Corporation CEO J. Craig Venter.
As importantly, the continued mining of cell theory and evolution of tissue culture exploded progress in cancer research and unlocked the mysteries of immunology, the workings of virology, the creation of a range of life saving vaccines from polio to mRNA cures for Covid, and much, much more.
Tags: anton van leewenhoek > canillo golgi > cell culture > cell theory > cells > ernst ruska > herb proctor > immortalized cell lines > in vitro > matthias schleiden > max knoll > ringers lactate > robert feulgen > robert Hooke > rudolph virchow > theodor schwann > tissue culture > walter flemming > william osler > william welch
The Most Profitable Convenience Store Product? Caffeinated, but not coffee.
Posted on | April 7, 2025 | Comments Off on The Most Profitable Convenience Store Product? Caffeinated, but not coffee.
Mike Magee

If you enter a Starbucks or Dunkin’ Donuts on any given day, it is more than likely that you will exit with roughly half the maximum recommended daily dosage of caffeine in a hot or cold coffee beverage. No surprise here.
But you may be surprised to know that your caffeine hit is likely to be just as high (or higher) if you visit a Convenience Market like 7-Eleven or Cumberland Farms, but not from a cup of coffee. This is because 1/3 of all beverage sales in these outlets is in the form of caffeine super-charged energy drinks. More on that in a moment.
Convenience stores, often associated with easy access gas pumps, are ubiquitous is most parts of our nation. Take the tiny state of Rhode Island. At last tally, it has 617 Convenience stores, and that’s an increase of 1 1/4 % over last year. 279 of these stores (45%) are single-owner operations.
Packaged beverages account for roughly 16% of sales. That’s second only to cigarette sales. And when it comes to profitability, beverages are #1, contributing a whopping 20% of gross dollar sales. And among all beverages, the leader of the pack in profit margins is – you guessed it – energy drinks at 44%.
Total U.S. sales of energy drinks in 2024 was nearly 22 billion dollars. These beverages come in variety of sizes, are usually canned and refrigerated, and are packed with extras.For example, one brand (Celsius) listed in the chart above includes the following additives: Citric Acid, Taurine (an amino acid),Green Tea extract, Ascorbic Acid (Vitamin C), the artificial sweetener Sucralose, the metabolite Glucuronolactone, ginger root extract, and of course a range of vitamins and artificial flavors.
To their young fans, taste is secondary to increased attention and reaction speed. These are due to the heavy dose of caffeine. Other promised effects, like increased muscle strength and endurance, are not supported by data. What has been well documented is that exceeding a daily dose of 400mg of caffeine can cause problems including cardiac irregularities, anxiety and panic disorders, and GI disturbances.
There are currently no federal age requirements for the purchase of energy drinks.
Tags: bang > caffeine > celsius > Energy Drinks > monster > performance drinks convenience stores > red bull > rockstar > teen health
The World’s Most Widely Used Psychoactive Drug?
Posted on | April 2, 2025 | Comments Off on The World’s Most Widely Used Psychoactive Drug?
Mike Magee
Question: What is the world’s most widely used psychoactive drug?
Answer: Caffeine
In the U.S., caffeine is consumed mainly in the form of coffee, tea, and cola. But coffee dominates. Worldwide, humans consume over 10 million tons of coffee beans a year. Roughly 16% (1.62 million tons) is devoured by Americans. The daily intake of caffeine varies depending on type of beverage and brand as the chart below indicates.
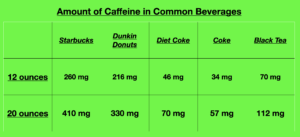
On average, each American consumes approximately 164 mg of caffeine each day. That’s roughly 1 small cup of Dunkin or (3.5) 12-ounce Diet Cokes (Trump consumes at least 12 cans of Diet Coke a day).
Across the globe, daily consumption of caffeine is close to universal. Eight in 10 humans consume a caffeinated beverage daily. That makes this chemical substance the “most commonly consumed psychoactive substance globally.” Its’ popularity is related to its ability to deliver three useful physiological enhancements – wakefulness, motor performance, and cognition.
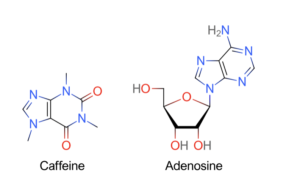
Chemically, caffeine is a close cousin of adenosine which is present in brain neurons. Adenosine builds up in synaptic connections between brain neurons. When it binds bind to special receptors, it activates neurons that promote sleepfulness. Ingested caffeine is water and lipid soluble, and therefore is able to traverse the blood-brain barrier. Once inside, its’ chemical structure mimics that of adenosine, and it occupies adenosine receptors because it shares the same approximate shape and size. When these receptors are occupied by caffeine, adenosine molecules are unable to activate the receptors. The net effect is wakefulness.
Caffeine passes thru small intestine cell walls and is absorbed within 45 minutes of ingestion. From there, it is distributed to all bodily cells reaching highest concentrations within 1-2 hours. The average time required to remove 1/2 of a caffeine dose (the half-life) is 3 to 7 hours. Thereafter it is broken down in the liver.
Over 30 plants species naturally produce caffeine. The most common source of caffeine are the seeds or beans of two coffee plants ( Coffee arabica and Coffee canephore), the leaves of tea plants, the seeds of the cocoa plant (Theobroma cacao) used in chocolate production, and kola nuts (used to produce Cola beverages).
For chocolate lovers, caffeine levels depend on the product. A 4 ounce bar of dark chocolate has approximately 80 mg of caffeine. Night time injesters may do better with milk chocolate which contains 24 mg in 4 ounces.
Pure solid caffeine is bitter, odorless, and melts at 235 degrees C. The 60’s generation were familiar with various tablet forms like No-Doz (Bristol-Myers Squibb) and Vivarin (SmithKline Beecham).. Each tablet contained 100 mg of caffeine. The U.S. market is estimated at $60 million annually. The three top consumer markets are college students (for “all-nighters”), truck drivers and body builders.
None of this is especially breaking news. The restorative powers of boiling tea leaves was first documented in 3000 BC. The Cocoa bean was harvested by Mayans in 600 BC. Coffee use is more recent, with first accounts in the Middle East in the 15th century. Three centuries later, French chemists isolated the active ingredients, with the term Caféine first appearing in the French scientific literature in 1822.
Back in 1911, Trump may have run into a problem ingesting 10 Cokes a day. Public officials viewed the product (and its stimulants) with suspicion. In fact, their seizure of 20 kegs of Coca-Cola syrup in Chattanooga, TN, led to the landmark case, United States v. Forty Barrels and Twenty Kegs of Coca-Cola. The company prevailed only to have the U.S. Congress pass a law the following year requiring that the company to include the phrase “habit-forming” on their label.
These days, caffeine consumption varies with age and sex – “2 mg/kg/day in children, 2.4 mg/kg/day in women, and 2.0 mg/kg/day in men.” As for caffeine powder tablets, they remain unregulated. Reading between the lines, experts are preaching caution a bit more often, as in this government summary in 2017:
“When taken together, the literature reviewed here suggests that ingested caffeine is relatively safe at doses typically found in commercially available foods and beverages. There are some trends in caffeine consumption, such as alcohol-mixed energy drinks, that may increase risk of harm. There are also some populations, such as pregnant women, children, and individuals with mental illness, who may also be considered vulnerable for harmful effects of caffeine. Excess caffeine consumption is increasingly being recognized by health-care professionals and by regulatory agencies as potentially harmful.”
Tags: adenosine > cafeine > caffeine > chocolate > coffee > Coke > green vs. black tea > No-Doz > tea > Vivarin > wakefulness
Vital Signs Are Vital: How We Learned To Measure Blood Pressure.
Posted on | April 1, 2025 | Comments Off on Vital Signs Are Vital: How We Learned To Measure Blood Pressure.
Mike Magee
It has been estimated that a medical student learns approximately 15,000 new words during the four years of training. One of those words is sphygmomanometer. the fancy term for a blood pressure monitor. The word is derived from the Greek σφυγμός sphygmos “pulse”, plus the scientific term manometer (from French manomètre).
While medical students are quick to memorize and learn to use the words and tools that are part of their trade, few fully appreciate the centuries long efforts, to advance incremental insights, discoveries, and engineering feats that go into these discoveries.
Most students are familiar with the name William Harvey. Without modern tools, he deduced from inference rather than direct observation that blood was pumped by a four chamber heart through a “double circulation system” directed first to the lungs and back via a “closed system” and then out again to the brain and bodily organs. In 1628, he published all of the above in an epic volume, De Motu Cordis.
Far fewer know much about Stephen Hales, who in 1733, at the age of 56, is credited with discovering the concept of “blood pressure.” A century later, the German physiologist, Johannes Müller, boldly proclaimed that Hales “discovery of the blood pressure was more important than the (Harvey) discovery of blood.”
Modern day cardiologists seem to agree. Back in 2014, the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure reported that “With every 20 mm Hg increase in systolic or 10 mm Hg increase in diastolic blood pressure, there is a doubling risk of mortality from both ischemic heart disease and stroke.”
But comparisons are toxic. No need to diminish Harvey who correctly estimated human blood volume (10 pints or 5 liters), the number of heart contractions, the amount of blood ejected with each beat, and the fact that blood was continuously recirculated – and did this all 400 years ago. But how to measure the function, and connect those measurements to an amazingly significant clinical condition like hypertension, is a remarkable tale that spanned two centuries and required international scientific cooperation.
Harvey was born in 1578 and died in 1657, twenty years before the birth of his fellow Englishman, Stephen Hales. Hales was a clergyman whose obsessive and intrusive fascination with probing the natural sciences drew sarcasm and criticism from the likes of classical scholar and sometimes friend, Thomas Twinning. He penned a memorable insult laced poem in Hales’ honor titled “The Boat of Hales.”
“Green Teddington’s serene retreat
For Philosophic studies meet,
Where the good Pastor Stephen Hales
Weighed moisture in a pair of scales,
To lingering death put Mares and Dogs,
And stripped the Skins from living Frogs,
Nature, he loved, her Works intent
To search or sometimes to torment.”

The torment line may be well justified in light of Hales own 1733 account of his historic first ever mention of the measurement of arterial blood pressure, illustrated and self-described here:
“In December I caused a mare to be tied down alive on her back; she was fourteen hands high, and about fourteen years of age; had a fistula of her withers, was neither very lean nor yet lusty; having laid open the left crural artery about three inches from her belly, I inserted into it a brass pipe whose bore was one sixth of an inch in diameter … I fixed a glass tube of nearly the same diameter which was nine feet in length: then untying the ligature of the artery, the blood rose in the tube 8 feet 3 inches perpendicular above the level of the left ventricle of the heart; … when it was at its full height it would rise and fall at and after each pulse 2, 3, or 4 inches.”
Having established the existence of “blood pressure,” the world would wait nearly another century to gain access to a reliable tool for measurement. That advance came from the hands of French physician-physicist, Jean Léonard Marie Poiseuille. He was born in 1799, amidst the flames of the French Revolution. In 1828, as a doctoral candidate, his dissertation on the use of a mercury manometer, attached to an anticoagulant laced cannula, in lab animal vessels as small as 2 mm in diameter, yielded measurable, and reproducible arterial pressure readings, earning him a gold medal from the Royal Academy of Medicine.
Carl Ludwig, a 31-year old German professor of physiology, next decided Poseuille needed a permanent and transportable record. His solution in 1847 was to attach a float with a writing pen to the open mercury column. As the mercury rose, the pen scratched out a reading on a revolving smoked drum.
But direct arterial puncture was impractical and invasive. By 1955, scientists had surmised that applying external counter pressure to an artery could obliterate the pulse below the obstruction, and that measuring the pressure generated by an obstructing external rubber ball would essentially reveal the blood pressure generated by a contracting heart – the systolic pressure.
In 1881, an Austrian physician named Karl Samuel Ritter von Basch created an elaborate portable machine that included a manometer capable of measuring the internal water pressure inside an inflatable rubber ball applied at the wrist to the radial artery. The pressure necessary to eliminate the pulse below was roughly the peak pressure of the column of blood when the heart contracted. Eight years later, the French physician, Pierre Carle Édouard Potain, replaced the water with air for compression.
By 1896, blood flow was appreciated as a series of waves that peaked when the heart contracted, and fell as the heart relaxed. The wrist compressing rubber rubber cup was replaced by an air filled cuff wrapped around the upper arm which constricted the larger brachial artery. A Russian surgeon, N.C. Korotkoff, in 1905, suggested that doctors listen to the waves rather than feel for the pulse. The sounds he described became known as Korotkoff sounds.

As described in a 1941 translation of the Russian paper and illustrated here by wikipedia, Korotkoff wrote, “On the basis of this observation, the speaker came to the conclusion that a perfectly constricted artery under normal conditions, does not emit any sounds…The sleeve is put on the middle third of the arm; the pressure in this sleeve rises rapidly until the circulation below this sleeve stops completely. At first there are no sounds whatsoever. As the mercury in the manometer drops to a certain height, there appears the first short or faint tones, the appearance of which indicates that part of the pulse wave of the blood stream has passed under the sleeve…Finally all sounds disappear. The time of disappearance of the sounds indicated the free passage or flow of the blood stream… Consequently, the reading of the manometer at this time corresponds to the minimum (diastolic) blood pressure.”
It is easy to forget, in an age of semiconductors, photocells and strain gauges, that progress in understanding the human circulatory system took centuries to acquire, and international cooperation. When Covid hit, homes that could acquired Home Blood Pressure Monitors and Pulse Oximeters that attached to an index finger and delivered oxygen saturation of blood and pulse with no delay. For a little more, you can access a Portable ECG monitor in the comfort of your own home.
We appear to have entered a new era, one where a U.S. president and his enablers are fast at work dismantling American scientific capacity and cooperative, AI-laced, international science discovery capacity. The timing couldn’t be worse, since increasingly, we patients are expected to enthusiastically participate as both providers and recipients of our own health care.
Tags: blood pressure > blood pressure monitor > ECG monitor > Jean Leonard Marie Poiseuille > Karl Samuel Ritter von Basch > Korotkoff sounds > N.C. Korotkoff > Pierre Carle Edouard Potain > pulse oximeter > sphygmomanometer > Stephen Hales > william harvey
"Code Blue INDEX online"

![]()
![]()
Prospective Health Blog
BIOGRAPHY
Homegrown Friends
BIOGRAPHY
NIH Precision Medicine
BIOGRAPHY
Health in 30
BIOGRAPHY
Larry's Letters
BIOGRAPHY
Precision Medicine, Euthanasia, Abortion, Communism, Trillions of Dollars, Losing Freedom, and Town Hall Mobs BIOGRAPHY
Yearning for Universal Coverage Is Not Universal
BIOGRAPHY

